
Research ArticleOpen Access, Volume 4 Issue 2
Myocardial infarction mortality in young Brazilian women, 2015-2024
Schnoeller Emilly Anne A1*; Lisboa BA1; Santos IJA1; Silva SP1; Pinheiro AO1; Gonçalves EES1; Sawabini ACL1; Freitas RAP1; Farias ES2; Feldman A3,4; Gun C4
1School of Medicine, Santo Amaro University (UNISA), São Paulo, Brazil.
2Federal University of ABC (Universidade Federal do ABC), Brazil.
3Department of Cardiology, Rede D’Or São Luiz Hospitals, Brazil.
4Instituto Dante Pazzanese de Cardiologia, São Paulo, Brazil.
*Corresponding author: Emilly Anne Schnoeller
School of Medicine, Santo Amaro University (UNISA), São
Paulo, Brazil.
Tel: +55-11-97265–1306;
Email: emilly.schnoeller@gmail.com
Received : Apr 26, 2026 Accepted : May 13, 2026 Published : May 20, 2026
Epidemiology & Public Health - www.jpublichealth.org
Copyright: Schnoeller EA © All rights are reserved
Citation: Schnoeller EA, Lisboa BA, Santos IJA, Silva SP, Pinheiro AO, et al. Myocardial infarction mortality in young Brazilian women, 2015-2024. Epidemiol Public Health. 2026; 4(2): 1100.
Abstract
Background: Cardiovascular diseases remain the leading cause of death in Brazil. Although traditionally associated with men and older ages, Acute Myocardial Infarction (AMI) has shown a progressive “rejuvenation” pattern, with growing impact among women in their productive years. Sex-specific clinical presentation, mechanistic heterogeneity (including spontaneous coronary artery dissection and ischemia with non-obstructive coronary arteries), and structural inequities in access to cardiovascular care converge to make young women a particularly vulnerable population. This study aimed to analyze the temporal trend and regional pattern of AMI mortality in women under 60 years of age in Brazil between 2015 and 2024.
Methods: Population-based, ecological time-series study using the Mortality Information System (SIM/ DATASUS). All deaths coded as ICD–10 I21 or I22 in women under 60 years between January 1, 2015 and December 31, 2024 were included. Variables analyzed comprised year of death, age group (5-year bands), and geographic macroregion. Descriptive statistics, proportions with 95% confidence intervals (Wilson method), Joinpoint Regression Analysis with Annual Percent Change (APC) and Average Annual Percent Change (AAPC) and crude mortality rates per 100,000 women-year using IBGE 2022 population projections as denominators were applied.
Results: A total of 66,907 deaths were recorded. Mortality concentrated in the 50-59 age group (62.2%), followed by 40–49 years (27.4%) and women under 40 years (10.4%). Joinpoint regression of the national series identified two statistically significant inflection points (2020 and 2022), partitioning the decade into three segments: 2015–2020 (APC –2.33%/yr, 95% CI –2.86 to –1.79; p< 0.001), 2020 2022 (post-pandemic rebound: APC +2.51%/yr, 95% CI +1.09 to +3.95; p< 0.001) and 2022–2024 (APC –3.78%/yr, 95% CI –5.35 to –2.19; p< 0.001), with an overall AAPC of –1.60%/yr (95% CI –2.16 to –1.04; p< 0.001). Age-stratified analysis revealed that only the 50–59 stratum showed a statistically significant overall decline (AAPC –1.26%/yr; p< 0.001), whereas mortality in women under 40 (AAPC –1.19%/yr; p=0.18) and 40–49 years (AAPC –0.49%/yr; p=0.37) remained essentially unchanged across the decade. The Southeast (45.9%) and Northeast (29.1%) macroregions concentrated the largest absolute burden, while population-adjusted crude rates were homogeneous across the Southeast, Northeast and South.
Conclusion: AMI mortality in young Brazilian women remains a substantial public health challenge. The statistically significant overall decline observed in the national series is driven exclusively by women aged 50–59 years; mortality in women under 50 has not declined significantly across the decade, providing direct quantitative evidence of the “rejuvenation” of AMI in this population. The Joinpoint discontinuities at 2020 and 2022 expose the vulnerability of cardiovascular surveillance during the COVID-19 pandemic. Sex-specific public health strategies focused on professional awareness of atypical symptoms, mitigation of regional disparities, and integration of female-specific cardiovascular risk into primary health care are urgently needed.
Keywords: Myocardial infarction; Women’s health; Mortality; Time-series studies; Public health; Cardiovascular diseases; Health inequities.
Abbreviations: AAPC: Average Annual Percent Change; AMI: Acute Myocardial Infarction; APC: Annual Percent Change; CI: Confidence Interval; CNS: National Health Council (Brazil); CVDs: Cardiovascular Diseases; DATASUS: Department of Informatics of the Unified Health System; IBGE: Brazilian Institute of Geography and Statistics; ICD-10: International Classification of Diseases, 10th Revision; MINOCA: Myocardial Infarction with Non-Obstructive Coronary Arteries; PHC: Primary Health Care; SCAD: Spontaneous Coronary Artery Dissection; SIM: Mortality Information System; SUS: Brazilian Unified Health System.
Introduction
Cardiovascular Diseases (CVDs) constitute the leading cause of mortality worldwide and in Brazil, with Acute Myocardial Infarction (AMI) representing one of the most lethal manifestations of the ischemic spectrum [1,2]. Although traditionally framed as a predominantly male and senile pathology, contemporary epidemiological evidence supports a progressive “rejuvenation” of AMI, with a concerning rise in incidence among women in their productive years [3,4]. This shift reflects the convergence of metabolic risk factors that disproportionately affect women, including the obesity epidemic, increasing prevalence of type 2 diabetes and metabolic syndrome, persistent tobacco uses among younger cohorts, and the cardiometabolic consequences of psychosocial stress and sedentary lifestyles [4,5].
Beyond classical risk factors, AMI in young women is characterized by clinical, mechanistic, and pathophysiological singularities that complicate timely recognition and treatment. Atypical symptomatic presentations — such as extreme fatigue, nausea, epigastric discomfort, dyspnea, and interscapular pain rather than classical retrosternal pain — frequently lead to delays in seeking care, underestimation of ischemic risk by both patients and clinicians, and reduced rates of timely reperfusion therapy when compared with men [6,7]. Furthermore, sex specific mechanisms of myocardial ischemia, including Spontaneous Coronary Artery Dissection (SCAD), microvascular dysfunction, and Myocardial Infarction with Non-Obstructive Coronary Arteries (MINOCA), are disproportionately prevalent in younger women and are systematically underdiagnosed when standard angiographic criteria are applied [8,9]. The cumulative effect of these factors is a sustained excess in case fatality among young women compared to age-matched men [6-9].
In Brazil, this clinical complexity is further amplified by structural inequities in access to cardiovascular care across the five macroregions, marked heterogeneity in the maturity of the chest pain network, and persistent gaps in primary prevention within the Unified Health System (SUS) [5,10]. The COVID-19 pandemic, beginning in 2020, added an additional and abrupt layer of complexity to cardiovascular surveillance: the fear of in-hospital contagion, the saturation of emergency services, and the reorganization of elective care collectively reduced the volume of acute coronary syndromes brought to medical attention, with documented increases in out-of-hospital and home-based cardiovascular deaths [11,12]. The downstream effect on official mortality records has been an underestimation of the true ischemic burden during 2020–2021, followed by an apparent rebound in subsequent years.
Despite the magnitude of the problem, contemporary national-level analyses of AMI mortality specifically targeting women under 60 years of age remain scarce. Existing literature predominantly focuses on aggregate adult populations, masking the unique trajectory of younger women and limiting the ability of public health authorities to design targeted interventions. Therefore, this study aimed to analyze the temporal trend and regional distribution of AMI mortality among women under 60 years of age in Brazil between 2015 and 2024, providing actionable epidemiological evidence to inform sex-specific public health policies, primary prevention strategies, and the strengthening of the cardiovascular care network within the SUS.
Materials and methods
Study design and ethical considerations
This is a population-based, ecological, time-series epidemiological study covering the ten-year period from January 1, 2015 to December 31, 2024. The ecological design was chosen as the most appropriate framework for the investigation of population-level mortality trends derived from secondary, fully aggregated, and de-identified administrative data, without interference in individual clinical practice or care decisions. Because the data source is publicly available, fully de-identified, and of an aggregated nature, the study was exempt from review by a Research Ethics Committee, in accordance with Article 1, Sole Paragraph, item III, of National Health Council (CNS) Resolution No. 510/2016 [13]. The study was reported in accordance with the STROBE statement for observational research.
Data source
Mortality data were extracted directly from the public TABNET interface of the Department of Informatics of the Unified Health System (DATASUS), which compiles records from the Mortality Information System (SIM) [14]. SIM is a nationwide, compulsory, and standardized notification system that aggregates death certificate information from the entire national territory and is widely recognized as the official source for mortality surveillance in Brazil. Population denominators for the calculation of mortality rates were obtained from the Brazilian Institute of Geography and Statistics (IBGE), using the most recent intercensal population projections by sex, age group, and macroregion [15].
Inclusion and exclusion criteria
All deaths recorded in SIM whose underlying cause was coded as I21 (acute myocardial infarction) or I22 (subsequent myocardial infarction) according to the International Classification of Diseases, 10th Revision (ICD–10) were included. The study population was restricted to female sex and age at death below 60 years. Records with missing information on age group, sex, or year of death were excluded from analysis to preserve the integrity of trend measures and regional comparisons. No imputation procedures were applied for missing data.
Variables analyzed
Data were tabulated by year of death, age group, and geographic macroregion. Age groups followed the standardized categorization available in TABNET: under 20 years, 20–29, 30–39, 40–44, 45–49, 50–54, and 55–59 years. For analytical and presentational purposes, age groups were also pooled into three broader strata: under 40 years, 40–49 years, and 50–59 years. The five Brazilian macroregions — North, Northeast, Central-West, Southeast, and South — were considered for the regional analysis. Data corresponding to the years 2023 and 2024 were included in the analysis with the explicit caveat of incompleteness, as they remain under consolidation by SIM/ DATASUS and may be subject to subsequent revision.
Statistical analysis
Descriptive statistics were used to characterize the distribution of deaths according to age group, year, and macroregion, with absolute and relative frequencies. Proportions were reported with 95% Confidence Intervals (CI) calculated by the Wilson score method, which is preferred over the normal approximation when proportions deviate from 0.5 or when the denominators differ markedly between strata. Crude mortality rates were calculated as the ratio between the number of deaths and the corresponding female population under 60 years of age, expressed per 100,000 women-year, using IBGE 2022 population projections as denominators.
The temporal trend was assessed using Joinpoint Regression Analysis (Joinpoint Regression Program, version 5.x; Statistical Methodology and Applications Branch, Surveillance Research Program, US National Cancer Institute), which is the methodological standard for time-series analysis in cancer and chronic-disease epidemiology and identifies statistically significant inflection points (“joinpoints”) in the trajectory of an outcome over time. The Annual Percent Change (APC) was estimated for each segment delimited by joinpoints, accompanied by 95% confidence intervals, and the Average Annual Percent Change (AAPC) was computed for the entire study period and stratified by age group and macroregion. The Monte Carlo permutation method was used to test the statistical significance of joinpoints, with a maximum of three joinpoints allowed and a minimum of two observations between adjacent joinpoints, in accordance with default recommendations of the program. Trends were classified as increasing, decreasing, or stable based on the direction and statistical significance of APC and AAPC estimates.
As a sensitivity analysis, an alternative trend evaluation was conducted using Prais–Winsten generalized least-squares regression, which corrects for first-order autocorrelation in time-series data, with significance assessed by the Durbin Watson statistic. To mitigate the analytical impact of pandemic related disruption on official records, an additional sensitivity analysis estimated the linear trend after excluding the pandemic years 2020 and 2021. All statistical tests were two-tailed, and a significance level of 5% (p< 0.05) was adopted. Analyses were performed using the Joinpoint Regression Program and the R statistical environment (version 4.x; R Foundation for Statistical Computing).
Results
Overall mortality and temporal pattern
Between January 1, 2015 and December 31, 2024, a total of 66,907 deaths from acute myocardial infarction were registered in SIM/DATASUS among women under 60 years of age in Brazil, corresponding to a national annual average of 6,691 deaths and a crude mortality rate of approximately 7.6 per 100,000 women-year using IBGE 2022 reference denominators. The annual time series displayed a heterogeneous trajectory across the decade (Figure 1, Figure 3, Table 3). A peak in absolute mortality was identified in 2016 (7,310 deaths), followed by a sustained decline through 2020 (6,211 deaths) — a cumulative relative reduction of 11.4% compared with 2015 and of 15.0% compared with the 2016 peak. After this nadir, mortality rebounded in 2021 (6,620 deaths) and 2022 (6,725 deaths), and resumed a downward trajectory in 2023 (6,476 deaths) and 2024 (6,247 deaths). When the entire decade was compared (2015 versus 2024), the net variation in absolute deaths was –10.9%.
Joinpoint regression of the national series identified two statistically significant joinpoints, at 2020 and at 2022, partitioning the decade into three biologically and historically interpretable segments (Figure 3). Between 2015 and 2020, mortality declined consistently with an Annual Percent Change (APC) of –2.33%/yr (95% CI –2.86 to –1.79; p< 0.001). Between 2020 and 2022, mortality reversed direction with an APC of +2.51%/yr (95% CI +1.09 to +3.95; p< 0.001), capturing the post pandemic rebound. From 2022 to 2024, mortality declined again at an accelerated rate (APC –3.78%/yr; 95% CI –5.35 to –2.19; p< 0.001). The Average Annual Percent Change (AAPC) for the full 2015–2024 period was –1.60%/yr (95% CI –2.16 to –1.04; p< 0.001), indicating a modest but statistically significant overall downward trend.
Distribution by age group
The age distribution of deaths showed a marked predominance in the 50–59 age group, which accounted for 62.2% of all events (95% CI 61.8–62.5%; n=41,599), followed by the 40–49 group (27.4%; 95% CI 27.1–27.8%; n=18,359) and women under 40 years of age (10.4%; 95% CI 10.2–10.6%; n=6,949) (Table 1). Within the 5-year age stratification (Figure 1), a clear monotonic gradient was observed, with the 55–59 stratum representing the largest single contributor to absolute mortality (37.1%; n=24,841). Despite this predominance, a consistent occurrence of events was registered in younger strata, with the under-40 group accounting for an annual mean of 695 deaths.
Age-stratified Joinpoint regression revealed a strikingly heterogeneous decade-long trajectory across age groups (Figure 4, Table 4). Only the 50–59 stratum exhibited a statistically significant overall decline (AAPC –1.26%/yr; 95% CI–1.93 to –0.58; p< 0.001), driven by a sustained reduction between 2016 and 2020 (APC –2.66%/yr; 95% CI –3.49 to –1.83; p< 0.001) followed by a slower decline thereafter (APC –0.97%/yr; 95% CI –1.84 to –0.09; p=0.030). In contrast, no statistically significant overall trend was observed in the 40–49 stratum (AAPC –0.49%/ yr; 95% CI –1.53 to +0.57; p=0.365) or in women under 40 years (AAPC –1.19%/yr; 95% CI –2.91 to +0.55; p=0.178). This stratified pattern provides direct quantitative support for the “rejuvenation” hypothesis of AMI in women: across an entire decade and 66,907 deaths, the established cardiovascular prevention strategies translated into a measurable mortality reduction only in women aged 50–59 years, while the burden in younger age groups remained essentially unchanged.
Regional distribution
The geographic distribution of AMI mortality showed a marked predominance in the Southeast macroregion, which concentrated 30,490 deaths (45.9%) over the decade, followed by the Northeast (19,303 deaths; 29.1%), South (7,816 deaths; 11.8%), Central-West (4,843 deaths; 7.3%), and North (3,978 deaths; 6.0%) (Figure 2A, Table 2). However, when the absolute burden was contextualized using the corresponding female population under 60 years from IBGE 2022 projections, the population-adjusted crude mortality rates per 100,000 women year were substantially more homogeneous across the Southeast, Northeast, and South regions (8.1, 8.2 and 8.3 per 100,000, respectively), while the Central-West (6.2) and, particularly, the North region (4.7) presented lower observed crude rates (Figure 2B, Table 2). This apparent paradox — a lower crude rate in the North despite well-documented structural inequities in access to cardiovascular care — should be interpreted with caution and likely reflects underdiagnosis, incompleteness of death certificates, and a higher proportion of deaths attributed to ill defined causes rather than a genuine epidemiological advantage.
Impact of the COVID-19 pandemic
The annual time series of total deaths revealed a discontinuity coinciding with the onset of the COVID-19 pandemic in 2020, statistically formalized by the joinpoint at that year (Figure 3). The 2020 nadir (6,211 deaths) represented a 7.7% decrease relative to 2019 and the lowest annual count of the entire decade. The subsequent rebound in 2021–2022 (APC +2.51%/ yr; p< 0.001) is consistent with a delayed mortality echo from cases incompletely captured during the acute pandemic phase, in line with international observations [11,12]. Notably, the post-rebound segment (2022–2024) displayed the steepest decline of the decade (APC –3.78%/yr; p< 0.001), suggesting either a partial recuperation of cardiovascular care delivery or the influence of the still-provisional 2024 data.
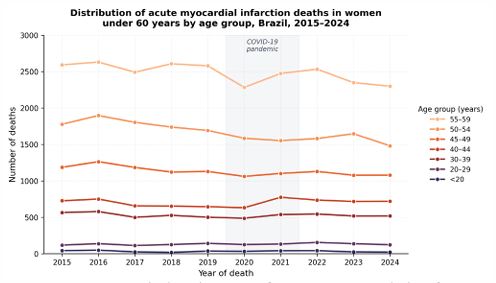
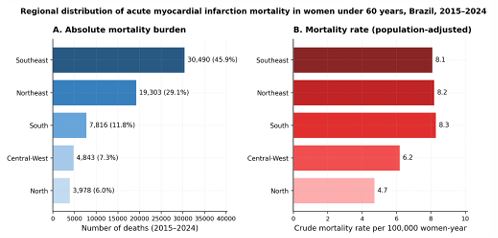
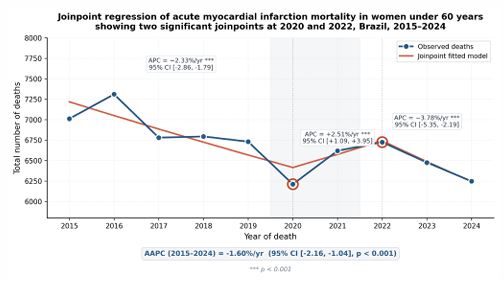
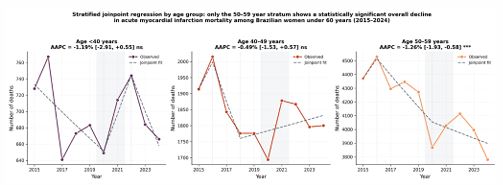
Table 1: Distribution of acute myocardial infarction deaths in women under 60 years of age, by age group, Brazil, 2015–2024.
| Age group (years) | Deaths (n) | % of total | 95% CI | Annual mean |
|---|---|---|---|---|
| <20 | 338 | 0.51% | 0.45–0.56% | 34 |
| 20–29 | 1,323 | 1.98% | 1.87–2.09% | 132 |
| 30–39 | 5,288 | 7.90% | 7.71–8.11% | 529 |
| 40–44 | 7,019 | 10.49% | 10.27–10.72% | 702 |
| 45–49 | 11,340 | 16.95% | 16.66–17.23% | 1,134 |
| 50–54 | 16,758 | 25.05% | 24.72–25.38% | 1,676 |
| 55–59 | 24,841 | 37.13% | 36.76–37.49% | 2,484 |
| Total (<60 years) | 66,907 | 100.0% | — | 6,691 |
Note: Data source: SIM/DATASUS, extracted by the authors via the TABNET interface. Confidence intervals (CI) for proportions calculated by the Wilson score method. Total decade burden = 66,907 deaths.
Table 2: Regional distribution of acute myocardial infarction deaths in women under 60 years of age, Brazil, 2015–2024.
| Region | Deaths (n) | % of total | 95% CI | Crude rate* |
|---|---|---|---|---|
| Southeast | 30,490 | 45.9% | 45.5–46.3% | 8.1 |
| Northeast | 19,303 | 29.1% | 28.7–29.4% | 8.2 |
| South | 7,816 | 11.8% | 11.5–12.0% | 8.3 |
| Central-West | 4,843 | 7.3% | 7.1–7.5% | 6.2 |
| North | 3,978 | 6.0% | 5.8–6.2% | 4.7 |
| Brazil | 66,430 | 100.0% | — | 7.7 |
Note: *Crude mortality rate per 100,000 women-year, calculated using IBGE 2022 population projections for women under 60 years as denominators. The discrepancy between the regional total (66,430) and the national figure (66,907) reflects rounding of regional percentages reported by SIM/DATASUS. Confidence intervals (CI) calculated by the Wilson score method.
Table 3: Annual distribution of acute myocardial infarction deaths in women under 60 years of age, Brazil, 2015–2024.
| Year | Deaths (n) | % of decade | Δ vs previous year | Notable event |
|---|---|---|---|---|
| 2015 | 7,012 | 10.5% | Reference | Baseline |
| 2016 | 7,310 | 10.9% | +4.2% | Decade peak |
| 2017 | 6,780 | 10.1% | –7.3% | — |
| 2018 | 6,795 | 10.2% | +0.2% | — |
| 2019 | 6,731 | 10.1% | –0.9% | — |
| 2020 | 6,211 | 9.3% | –7.7% | Joinpoint #1; pandemic |
| 2021 | 6,620 | 9.9% | +6.6% | Pandemic rebound |
| 2022 | 6,725 | 10.1% | +1.6% | Joinpoint #2; rebound peak |
| 2023 | 6,476 | 9.7% | –3.7% | Post-rebound decline |
| 2024 | 6,247† | 9.3% | –3.5% | Provisional data |
| Total | 66,907 | 100.0% | –10.9% (2015 vs 2024) |
— |
Note: † Data for 2024 are still subject to revision by SIM/DATASUS at the time of analysis. The two highlighted years correspond to the joinpoints identified by the segmented Poisson regression of the national series (Figure 3, Table 4).
Table 4: Joinpoint regression analysis of acute myocardial infarction mortality in women under 60 years of age, Brazil, 2015 2024.
| Stratum | Period | APC (%) | 95% CI | p-value | Sig. |
|---|---|---|---|---|---|
| National (all <60 y) | 2015–2020 | –2.33 | [–2.86; –1.79] | < 0.001 | *** |
| 2020–2022 | +2.51 | [+1.09; +3.95] | < 0.001 | *** | |
| 2022–2024 | –3.78 | [–5.35; –2.19] | < 0.001 | *** | |
| AAPC 2015–2024 | Full period | –1.60 | [–2.16; –1.04] | < 0.001 | *** |
| Age <40 years | 2015–2020 | –2.33 | [–4.00; –0.64] | 0.007 | ** |
| 2020–2022 | +6.92 | [+2.44; +11.59] | 0.002 | ** | |
| 2022–2024 | –6.00 | [–10.60; –1.17] | 0.015 | * | |
| AAPC 2015–2024 | Full period | –1.19 | [–2.91; +0.55] | 0.178 | ns |
| Age 40–49 years | 2015–2016 | +4.42 | [–1.65; +10.88] | 0.157 | ns |
| 2016–2018 | –6.16 | [–8.63; –3.61] | < 0.001 | *** | |
| 2018–2024 | +0.67 | [–0.18; +1.52] | 0.124 | ns | |
| AAPC 2015–2024 | Full period | –0.49 | [–1.53; +0.57] | 0.365 | ns |
| Age 50–59 years | 2015–2016 | +3.32 | [–0.45; +7.23] | 0.085 | ns |
| 2016–2020 | –2.66 | [–3.49; –1.83] | < 0.001 | *** | |
| 2020–2024 | –0.97 | [–1.84; –0.09] | 0.030 | * | |
| AAPC 2015–2024 | Full period | –1.26 | [–1.93; –0.58] | < 0.001 | *** |
Note: APC, annual percent change; AAPC, average annual percent change; CI, confidence interval. Joinpoint locations were selected by minimum Bayesian Information Criterion (BIC) over a search of zero, one and two joinpoints with a minimum of two observations per segment. APC and AAPC obtained from a log-linear (Poisson) segmented regression of yearly counts; 95% CIs computed by the delta method on segment slopes. AAPC computed as the segment length–weighted average of segment slopes. Statistical significance: ***p< 0.001; **p< 0.01; *p< 0.05; ns, not significant. Boldface indicates the only age group with a statistically significant overall AAPC across the decade.
Discussion
The analysis of AMI mortality in women under 60 years of age in Brazil reveals an epidemiological landscape that challenges the traditional perception of cardiovascular disease as a predominantly male or senile pathology. The 66,907 deaths registered between 2015 and 2024 — approximately one death every 79 minutes — underscore the urgent need for sex-specific secondary prevention strategies aimed at the female population in the reproductive years and early climacteric, as well as for a structural reframing of cardiovascular risk perception in primary health care [1-4].
Statistical evidence of the “rejuvenation” phenomenon
The age-stratified Joinpoint analysis provides what is, to our knowledge, the most direct quantitative evidence to date of the “rejuvenation” phenomenon of acute myocardial infarction in Brazilian women. Across an entire decade and 66,907 deaths, only women aged 50–59 years showed a statistically significant overall decline in mortality (AAPC –1.26%/yr; p< 0.001). In women under 50, the decade-long average annual percent change was not significantly different from zero, with point estimates of –1.19%/yr in the under-40 stratum (p=0.18) and –0.49%/yr in the 40–49 stratum (p=0.37). This dissociation between age groups is not subtle: the established cardiovascular prevention apparatus that has been measurably effective in older women has yielded no measurable mortality benefit in women below the menopausal transition, despite the same decade of exposure to public health interventions, expansion of the Family Health Strategy, and refinement of cardiovascular guidelines. The biological and clinical heterogeneity of AMI in young women — including the higher prevalence of SCAD, MINOCA, and microvascular dysfunction discussed below — plausibly contributes to this differential, in interaction with persistent diagnostic delays.
Diagnostic barriers and atypical symptomatology
Although the highest absolute concentration of deaths was observed in the 50–59 age group, the persistence of approximately 10% of deaths among women under 40 and the absence of a significant downward trend in the 40–49 stratum across the decade is particularly concerning. They suggest that current cardiovascular prevention strategies, calibrated for the male and older female population, are insufficient for younger women. Unlike the classical male presentation, AMI in young women frequently manifests through atypical symptoms — extreme fatigue, nausea, epigastric pain, dyspnea, and interscapular discomfort — rather than classical retrosternal pain [6,7]. This non-classical phenotype contributes to delayed care-seeking, lower rates of pre-hospital electrocardiogram acquisition, lower rates of timely thrombolysis or primary angioplasty, and consequently higher in-hospital case-fatality compared to age-matched men [6-9].
In addition, sex-specific pathophysiological mechanisms substantially modify the clinical and prognostic profile of AMI in this population. Spontaneous Coronary Artery Dissection (SCAD) accounts for up to 35% of AMIs in women under 50 and is the leading cause of pregnancy-associated AMI, yet remains widely underdiagnosed when conventional angiographic criteria are applied [8]. Similarly, Myocardial Infarction with non-Obstructive Coronary Arteries (MINOCA) and coronary microvascular dysfunction are disproportionately prevalent in young women and are associated with non-trivial long term mortality despite the absence of obstructive disease [9]. Recognition of these sex-specific entities should be incorporated into national cardiovascular protocols and into the continuing education of emergency and primary-care physicians.
Hormonal and reproductive determinants
The reproductive trajectory of women modulates cardiovascular risk in ways not adequately captured by traditional risk-stratification tools. Premature menopause (before age 40), early menopause (40–44 years), preeclampsia, gestational diabetes, polycystic ovary syndrome, and combined hormonal contraceptive use (particularly in association with smoking) are independent or modifying determinants of cardiovascular risk in young women [4]. The persistent burden of mortality in the 30–49 age range observed in our series reinforces the need to integrate reproductive history into cardiovascular risk assessment within primary health care, in line with contemporary recommendations from the American Heart Association and the European Society of Cardiology.
Disruptive impact of the COVID-19 pandemic
One of the most striking findings of the present study was the atypical and abrupt drop in mortality observed in 2020 (6,211 deaths), which interrupted the relative stability that followed the 2016 peak. This phenomenon, also documented in high-income settings, does not reflect a true reduction in AMI incidence but rather a complex combination of reduced care-seeking behavior, hospital saturation, redirection of cardiovascular workforce to COVID-19 care, and changes in death-certificate practices [11,12]. The fear of in-hospital contagion and the overload of emergency services are believed to have produced an excess of out-of-hospital cardiovascular deaths, often coded as ill-defined or attributed to respiratory complications. The post-pandemic rebound observed in 2021 and 2022 is consistent with a delayed mortality echo from undertreated or unrecognized acute coronary events during the acute phase. This finding has structural implications for cardiovascular surveillance during future health emergencies, including the need for redundant chest-pain pathways and resilient referral networks.
Regional inequities and the role of primary care
The disparity between the absolute burden in the Southeast and Northeast and the lower observed values in the North and Central-West regions reflects, in large measure, the structural inequities of health care delivery in Brazil and the demographic concentration of the female population in the southern half of the country. While the Southeast and South regions have a denser primary care network, broader access to high-complexity hemodynamics centers, and shorter pre-hospital times for primary angioplasty, the North region faces well-documented logistical barriers, geographic dispersion, and a chronic shortage of cardiovascular specialists [10]. The lower observed crude mortality in the North, despite these structural disadvantages, is unlikely to represent a genuine protective profile and more plausibly reflects a combination of underdiagnosis, deficient death-certificate completion, and a higher proportion of deaths attributed to ill-defined causes.
In all regions, primary health care occupies a central role in cardiovascular prevention through control of hypertension, diabetes, dyslipidemia, smoking cessation, and the systematic identification of women with sex-specific risk factors. Strengthening of the Family Health Strategy, integration of reproductive history into cardiovascular risk assessment, and the implementation of regional chest-pain protocols sensitive to female symptomatology are critical levers for reducing premature mortality in this population.
Strengths and limitations
The principal strengths of this study include its national coverage, the use of an official and standardized administrative data source (SIM/DATASUS), the ten-year analytical horizon, and the explicit use of methodological standards for time series analysis. The integrated regional, age-stratified, and temporal perspective allows for the identification of inequities and inflection points that would otherwise be obscured by aggregate national figures.
Several limitations should be acknowledged. First, as an ecological study, our analysis cannot establish individual-level causality and is susceptible to ecological fallacy. Second, the data for 2023 and 2024 remain provisional and may be revised by SIM/DATASUS after final consolidation, which may alter the most recent segments of the trend. Third, mortality registry data are subject to misclassification and underreporting, particularly in regions with limited death-certificate completeness, which may artificially deflate the crude rates observed in the North and Central-West. Fourth, crude mortality rates were not age standardized in the present analysis; future work using direct standardization to a reference population (e.g., the WHO World Standard Population) is recommended for more refined inter regional comparisons. Fifth, the study did not address case fatality, hospitalization rates, or the specific contribution of SCAD and MINOCA, which require linkage to hospitalization databases (SIH/SUS) and clinical registries.
Conclusion
Although the absolute number of AMI deaths in young Brazilian women has shown periods of relative stability across the 2015–2024-decade, mortality from acute myocardial infarction in this population remains a substantial public health challenge. The atypical fluctuations observed during the COVID-19 pandemic exposed the vulnerability of cardiovascular surveillance and care during health crises, while the persistent mortality burden in younger strata signals critical gaps in primary prevention, sex-specific risk perception, and timely access to evidence-based cardiovascular care.
The findings of this study support the need for sex-specific public health policies and clinical protocols tailored to the female population, with particular emphasis on professional awareness of atypical symptomatology, integration of reproductive history into cardiovascular risk assessment, expansion of structured chest-pain networks throughout the SUS, and dedicated cardiovascular surveillance strategies designed to remain resilient in the face of future health emergencies. Continued investment in standardized national surveillance, alongside the development of female-specific clinical registries for SCAD, MINOCA, and pregnancy-associated coronary events, will be essential to translate these epidemiological signals into measurable reductions in premature cardiovascular mortality among Brazilian women.
Declarations
Conflicts of interest: The authors declare that there are no conflicts of interest regarding the publication of this manuscript.
Funding: This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Acknowledgement: The authors thank the School of Medicine of Santo Amaro University (UNISA) and the Cardiology League of UNISA for their institutional support.
References
- Mansur AP, Favarato D. Mortality from cardiovascular diseases in Brazil and across the world. Arq Bras Cardiol. 2021; 117: 1061 1071.
- World Health Organization. Cardiovascular diseases (CVDs) fact sheets [Internet]. Geneva: WHO; 2023 [cited 2026 Apr 21]. Available from: https://www.who.int/news-room/fact-sheets/ detail/cardiovascular-diseases-(cvds)
- Précuma JE, Bertolami A, Pereira AC, Lottenberg AM, Issa JS, Ferreira JFM, et al. Diretriz Brasileira de Prevenção Cardiovascular. Arq Bras Cardiol. 2019; 113: 787-891.
- Wenger NK, Lloyd-Jones DM, Elkind MSV, Fonarow GC, Warner JJ, Alger HM, et al. Call to action for cardiovascular disease in women: epidemiology, awareness, access, and delivery of equitable health care: a presidential advisory from the American Heart Association. Circulation. 2022; 145: e1059-e1071.
- Schmidt MI, Duncan BB, Azevedo e Silva G, Menezes AM, Monteiro CA, Barreto SM, et al. Chronic non-communicable diseases in Brazil: burden and challenges. Lancet. 2011; 377: 1949-1961.
- Mehta LS, Beckie TM, DeVon HA, Grines CL, Krumholz HM, Johnson MN, et al. Acute myocardial infarction in women: a scientific statement from the American Heart Association. Circulation. 2016; 133: 916-947.
- Bairey Merz CN, Pepine CJ, Walsh MN, Fleg JL. Ischemia and no obstructive coronary artery disease (INOCA): developing evidence-based therapies and research agenda for the next decade. Circulation. 2017; 135: 1075-1092.
- Hayes SN, Kim ESH, Saw J, Adlam D, Arslanian-Engoren C, Economy KE, et al. Spontaneous coronary artery dissection: current state of the science: a scientific statement from the American Heart Association. Circulation. 2018; 137: e523-e557.
- Tamis-Holland JE, Jneid H, Reynolds HR, Agewall S, Brilakis ES, Brown TM, et al. Contemporary diagnosis and management of patients with myocardial infarction in the absence of obstructive coronary artery disease: a scientific statement from the American Heart Association. Circulation. 2019; 139: e891-e908.
- Ribeiro AL, Duncan BB, Brant LCC, Lotufo PA, Mill JG, Barreto SM. Cardiovascular health in Brazil: trends and perspectives. Circulation. 2016; 133: 422-433.
- Garcia S, Albaghdadi MS, Meraj PM, Schmidt C, Garberich R, Jaffer FA, et al. Reduction in ST-segment elevation cardiac catheterization laboratory activations in the United States during COVID-19 pandemic. J Am Coll Cardiol. 2020; 75: 2871 2872.
- De Rosa S, Spaccarotella C, Basso C, Calabro MP, Curcio A, Filardi PP, et al. Reduction of hospitalizations for myocardial infarction in Italy in the COVID-19 era. Eur Heart J. 2020; 41: 2083-2088.
- Brasil. Conselho Nacional de Saúde. Resolução nº 510, de 07 de abril de 2016. Diário Oficial da União. 2016 May 24; Seção 1: 44 46.
- Brasil. Ministério da Saúde. Departamento de Informática do SUS (DATASUS). Sistema de Informações sobre Mortalidade (SIM) [Internet]. Brasília: Ministério da Saúde; 2024 [cited 2026 Apr 21]. Available from: http://tabnet.datasus.gov.br/
- Instituto Brasileiro de Geografia e Estatística (IBGE). Projeções da população do Brasil e Unidades da Federação, por sexo e idade: 2010-2060 [Internet]. Rio de Janeiro: IBGE; 2024 [cited 2026 Apr 21]. Available from: https://www.ibge.gov.br/