
Research ArticleOpen Access, Volume 4 Issue 2
Barriers to utilization of focused antenatal care among women attending maternal child health at Chiga Health Centre, Kisumu, Kenya
Redemptah Yeda1*; Elekiah Anguko2; Caroline Ouma2; Wilbroda Nancy Makunda3
1School of Public Health, Jomo Kenyatta University of Agriculture and Technology, Nairobi, Kenya.
2Department of Diagnostic and Laboratory Systems Program, Center for Disease Control, Kisumu, Kenya.
3Uzima University, Kisumu, Kenya.
*Corresponding author: Redemptah Yeda
School of Public Health, Jomo Kenyatta University of Agriculture and Technology, Nairobi, Kenya.
Email: Wakiored@gmail.com
Received : Mar 11, 2026 Accepted : Apr 26, 2026 Published : Apr 30, 2026
Epidemiology & Public Health - www.jpublichealth.org
Copyright: Yeda R © All rights are reserved
Citation: Yeda R, Anguko E, Ouma C, Makunda WN. Barriers to utilization of focused antenatal care among women attending maternal child health at Chiga Health Centre, Kisumu, Kenya. Epidemiol Public Health. 2026; 4(2): 1098.
Abstract
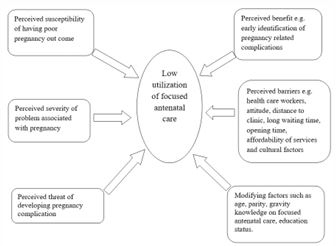
Focused Antenatal Care (FANC) is pivotal to reducing maternal and neonatal morbidity and mortality by enabling timely risk detection and management. Despite its importance, FANC utilization remains suboptimal in Kenya, particularly in Kisumu County. This cross-sectional study assessed barriers to FANC utilization among 138 pregnant women attending Maternal Child Health services at Chiga Health Centre between April - July 2023. The study identified key barriers including inadequate knowledge of FANC, long waiting times, transportation challenges, cultural beliefs, negative healthcare provider attitudes, and financial constraints. Multivariate analysis revealed knowledge deficits (AOR=2.5), transport difficulties (AOR=1.8), and poor provider attitudes (AOR=1.9) as significant predictors of low FANC uptake. Addressing these barriers through comprehensive community education, health system improvements, and provider training is essential to enhance FANC utilization and improve maternal outcomes in Kisumu.
Keywords: Focused antenatal care; Barriers; Maternal health; Antenatal care utilization; Kisumu; Kenya.
Introduction
Globally, the utilization of Antenatal Care (ANC) services has improved over the past decades due to increased maternal health initiatives and global commitments such as the Sustainable Development Goals; however, significant disparities persist between high-income and low-income countries, with women in low-income settings experiencing lower access and utilization of maternal health services [1]. Maternal mortality remains a significant public health challenge in sub-Saharan Africa, with Kenya reporting an estimated maternal mortality ratio of 342 per 100,000 live births [2]. The World Health Organization (WHO) recommends Focused Antenatal Care (FANC), entailing at least four quality visits during pregnancy, to timely identify and mitigate risks [3]. Despite policy efforts, FANC completion rates are low in rural and peri-urban Kenyan settings, including Kisumu County (Manyeh et al. 2020). Barriers to FANC are multifactorial—spanning individual, socio-cultural, and health system domains—and vary by locality [4]. This study sought to identify specific barriers to FANC utilization at Chiga Health Centre, Kisumu, to inform tailored interventions.
Methods
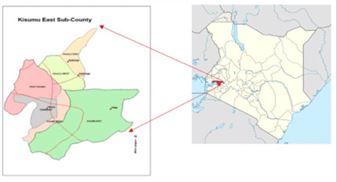
Study area
Kisumu East Sub-County, part of Kisumu County, is an administrative unit characterized by a mix of peri-urban and rural settings near Lake Victoria. Based on 2025 projections, the broader Kisumu metro area shows a population of approximately 422,000 [2]. It is characterized by subsistence farming and emerging industrial activities making it the third smallest district in the country the predominant religion in the district is Christianity with luo as the main ethnic group. Overall Chiga has low education attainment.
Study population
The recruitment period for the study was from mid-April to July 2023 the study recruited 138 participants. Kisumu population in the urban is estimated around 440,906, rural population is estimated 714,668 the total population is approximately 1,155,574.
Study design
This was a cross-sectional study, a questionnaire tool was used to collect data. The questionnaire for participating mothers was designed to collect information on knowledge of FANC, also to assess demographic and socio-cultural factors that contributed to low utilization of FANC. The health workers questionnaire captured current practices as well as perception towards FANC.
Sample size determination
In order to estimate the proportion of women who would make fewer than required number of FANC visits to within 10% of true population proportion with 95% confidence
Where: p = Prevalence (10%), z=level of confidence, q=statistical error, n=number of women participants. The number of pregnant women required was calculated using the formula (Cochran, W. G. (1977).
Where z = 1.96

n = 138
Thus 138 participants will be required in the study
Sampling techniques
Convenient sampling was employed to collect quantitative data for different variables at a given point of time.
Inclusion and exclusion criteria
All female of the reproductive age (15-45) years attending maternal child health at Chiga health centre, pregnant women above 35 weeks of gestation who are waiting to deliver at the facility were invited in the study. Potential mothers were not excluded based on religion, ethnicity, parity, gravidity and age. Women who didn’t give consent to participate.
Ethical consideration
Ethical consideration was approved from Jaramogi Teaching and Referral Hospital, verbal consent was obtained from both participating mothers and the health care workers. To maintain confidentiality for participating mothers, health workers used coded serial numbers instead of real names on the questionnaire.
Data management
Data was checked for completeness of information by the researcher once received from the health facility. The corrected data sheets were serially numbered by the researcher. The checked questionnaires were kept by the researcher ready for data processing and analysis.
Data analysis
Data was analysed using R software version 4.5.2. Statistical significance, evaluated at 0.05 levels. Frequencies and percentages were generated from the categories, and the mean percentage of were calculated to provide a general perception. The cut-off point of 50%, so that above 50 will denote positive perception and below denoting negative.
Results
Demographic factors
A total of 14.4% of the participant’s year’s ranged within 16 20 years, 43.4% were within the age range of 21-25 years, and 28.9% within the range of 26-30 years.
The mean age of participant’s women was 27.8 years (SD±5.4). Most were married (72%), had primary or no formal education (65%), and were unemployed or engaged in informal work (60%). Only 42% attended the recommended four or more FANC visits; many initiated ANC late (Table 1).
Table 1: Demographic characteristic of participating mothers.
| Age | n % |
|---|---|
| 16-20 | 20 (14.4%) |
| 21-25 | 60 (43.4%) |
| 26-30 | 40 (28.9%) |
| 31-35 | 10 (7%) |
| 36-40 | 4 (2.8%) |
| 41-45 | 4 (2.8%) |
| Marital status | |
| Married | 90 (65.2%) |
| Single | 30 (21.7%) |
| Divorced | 10 (7.2%) |
| Widowed | 8 (5.7%) |
Socio-cultural factors
Only 50% of women had given birth once, and only 26.8% were primi-gravid women. Parity was significantly inversely associated with number of visits to the FANC (P=0.01), those with first pregnancy were more likely to have visited FANC for more than 4 times compared to those who have ever had pregnancies. Participating women who reported that they seek permission before visiting FANC were very likely to make less than required (4) visits to the FANC (P=0.001). Those who reported personal reason (just not wanting to make lots of visits) were also significantly less likely to attend FANC (P=0.007). Some of the participating mothers who made less than four visits reported help of midwifes negatively affected the number of visits (Table 2).
Table 2: Socio-cultural factors.
| Variables | <4 visits % | >4 visits % | P-value |
|---|---|---|---|
| Parity | |||
| No child | 30(21.7%) | 15(36.5%) | |
| One or more children | 108(78.2) | 26(63.4%) | P=0.017 |
| Gravidity | |||
| Primi gravid | 26(18%) | 11(26.8%) | P=0.133 |
| Multi gravid | 112(81%) | 30(73%) | |
| Waiting to get permission from husbands | 115(83%) | 23(17%) | 0.007 |
| Never wanted to make lot of visits | 121(88%) | 17(12%) | 0.007 |
| Male involvement | 97(70%) | 41(30%) | 0.660 |
Knowledge on FANC
Despite high awareness (96%) and substantial attendance (80-90%), delays in gestational age at ANC initiation persist, limiting optimal FANC utilization. Strengthening community education focused on early booking and addressing systemic barriers remain key to improving maternal health outcomes in Kisumu County (Table 3).
Table 3: Knowledge on focused antenatal care.
| Variables | n % |
|---|---|
| Knowledge of FANC | 132(96%) |
| Attending mothers | 110(80%) |
| Antenatal visits | 124(90%) |
| Attendance of FANC | 117(80%) |
| Gestation age of initiation: | |
| 0 months 3 months | 28(20%) |
| 4 months 6 months | 97(70%) |
| 7 months 9 months | 13(10%) |
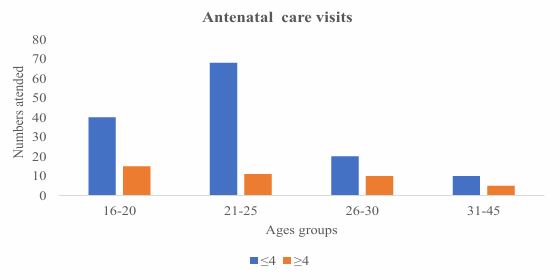
The younger women aged 16-20 years have 15 attending ≥4 visits, while women aged 31-45 years have only 5 attending ≥4 visits. Despite fewer women in the 31-45 age group overall, the proportion of women attending ≥4 visits are relatively similar or somewhat lower compared to younger groups (Figure 3).
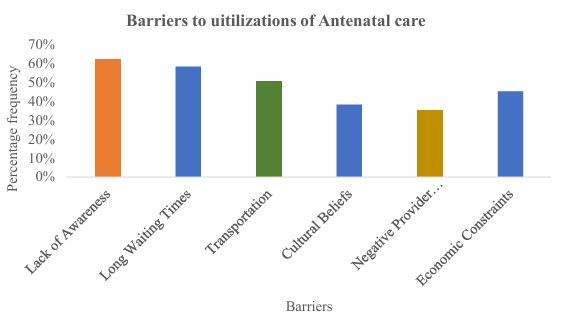
Barriers identified: Multivariate analysis highlighted lack of knowledge (AOR=2.5; 95% CI: 1.5-4.3), transportation challenges (AOR=1.8; 95% CI: 1.1-3.0), and negative provider attitudes (AOR=1.9; 95% CI: 1.2-3.2) as significant predictors of poor FANC utilization (Figure 4).
Health care worker training and current practices
A total of 10 health care workers participated in the study 10(100%) all had undergone training in reproductive health, whether formal or informal kind of training. 9(97%) and 9(95%) had been trained on Safe motherhood and FANC respectively. All the nurses who were trained on FANC said that they remem bered what they have been taught during the training (Table 4).
Care workers in regard to reproductive health and FANC
Table 4: Training, knowledge gained from FANC and current practices of health.
| Category | n% |
|---|---|
| Training: | |
| Reproductive training | 10(100%) |
| Safe mother hood training | 9(90%) |
| Focused antenatal training | 9(90%) |
| Knowledge gained from FANC training | 9(90%) |
| Current practices (information and services provided to pregnancy mother) | 10(100%) |
| Information regarding danger signs in pregnancy given to women | 10(100%) |
| FANC implementation was perceived positively | 9(90%) |
| Individualized health education | 7(70%) |
| Pregnant women are satisfied with the 4 visits | 8(80%) |
| Pregnant women are satisfied with the FANC services | 8(80%) |
Discussion
Age distribution: This study findings indicates that the majority of respondents are young adults, with 43.4% aged 21-25 and 28.9% aged 26-30. This concentration of younger individuals aligns with recent research suggesting that young adults often represent a significant proportion in studies related to workforce, education, and social behavior [5]. The smaller representation of older age groups (31 and above) reflects demographic trends where younger populations are more engaged in research participation or targeted in specific research contexts [6].
Marital status: The finding that 65.2% of respondents are married is consistent with studies showing high marriage rates in certain cultural or regional contexts despite global trends of delayed marriage [7]. The presence of 21.7% single individuals and smaller percentages of divorced and widowed participants is reflective of changing marital patterns, including increasing divorce rates and longer singlehood among younger generations [8]. The predominance of young married adults suggests the sample may represent a demographic in early family formation stages, which is an important factor in understanding social and economic behaviors [9]. The limited older age representation may indicate the need for targeted strategies to engage these groups in future studies [10].
Parity and number of visits: The difference in parity distributions between the two groups is statistically significant (P=0.017), suggesting that women without children are more likely to attend 4 or more visits compared to women who already have children. This aligns with findings from recent studies indicating that first-time mothers or those without children tend to have higher utilization of antenatal or health care services due to increased caution or perceived need for care [11,12]. This study finding aligns with global evidence Studies from various regions including Sub-Saharan Africa, South Asia, and Latin America consistently report that primiparous women (first-time mothers) are more likely to attend the recommended number of antenatal visits compared to multiparous women [11] (Tarekegn et al. 2021). This trend is often attributed to increased anxiety and awareness about pregnancy risks during the first pregnancy, motivating these women to seek more care.
Gravidity and number of visits: This indicates that previous pregnancy experience does not strongly influence the frequency of visits, a finding echoed by recent research indicating that other factors, such as cultural beliefs or partner support, may play a more pivotal role [13]. Globally, studies have reported mixed results. While some show primigravida women attend more visits [14], others have found gravidity to be less predictive than sociodemographic or cultural factors (Moller et al. 2021). This suggests that context plays a key role, with gravidity interacting variably with other barriers or facilitators.
Waiting to get permission from husbands: There is a highly significant difference in waiting to get permission from husbands between groups (< 4 visits: 83%; ≥4 visits: 17%; P=0.007). This suggests that women who delay or limit visits due to waiting for spousal permission are less likely to attend the recommended number of visits. This finding is consistent with recent literature emphasizing the critical role of gender dynamics and decision making power within households in influencing health care utilization [15,16].
Never wanted to make a lot of visits: Similarly, a substantial proportion of women in the < 4 visits group report never wanting to make many visits (88%) compared to only 12% in the ≥4 visits group, with a significant P-value of 0.007. This suggests personal preference or cultural attitudes towards health visits affect attendance. Such attitudes have been identified as barriers in several recent studies, underscoring the need for targeted health education to address misconceptions or resistance [17].
Male involvement: Male involvement did not significantly differ between groups (P=0.660), with 70% in the < 4 visits group and 30% in the ≥4 visits group reporting male involvement. Although male partner involvement is widely recognized as beneficial for maternal health outcomes, in this study it did not significantly correlate with the number of visits. This indicates that male involvement alone is insufficient without broader social and systemic support, as suggested by recent studies recommending integrated interventions to enhance male engagement more effectively [18].
Knowledge of FANC: A substantial majority (96%) of the participants demonstrated knowledge about FANC. Suggesting health education efforts regarding antenatal care have largely succeeded in disseminating key information within the population [19] (Manyeh et al. 2020).
Attending mothers & antenatal visits: 80% of mothers attended antenatal care, with 90% indicating some antenatal visits, suggesting generally good engagement with maternal health services. However, only 80% attended FANC specifically, indicating a gap between general ANC attendance and focused, goal-directed visits recommended by WHO (Manyeh et al. 2020) [19].
Gestational age at initiation: Early initiation (0-3 months) was low (20%), reflecting delayed entry into antenatal services for most women. A majority (70%) began ANC between 4-6 months, which limits early detection of pregnancy risks and reduce the number of visits feasible before delivery. Late initiation (7-9 months) occurred in 10% of women, heightening risk of missed interventions (Manyeh et al. 2020) [19]. While knowledge levels are high delayed initiation and incomplete adherence to recommended FANC visits persist. This delay in booking ANC could be linked to barriers such as economic constraints, cultural beliefs, or healthcare system challenges (long waiting times, provider attitudes) [4,20]. Early initiation of ANC is critical to allow the recommended minimum four focused visits, enabling timely risk assessment and management [3]. This data suggests need for targeted interventions encouraging earlier ANC booking and continuous engagement throughout pregnancy.
Antenatal care: Younger women were more receptive to antenatal care education and emphasize adherence to recommended visits, potentially influenced by increased health messaging targeting youth or first-time pregnancies [19] (Manyeh et al. 2020). Older women relied on previous pregnancy experiences and perceive less need for frequent visits, thus attending fewer FANC sessions [4]. Cultural beliefs and economic or logistic barriers identified in the study—such as transport challenges and negative provider attitude disproportionately affected older women who often have heavier household or economic responsibilities, limiting their availability for frequent visits [3,20]. Additionally, awareness levels and motivation for FANC decline with age or parity, contributing to lower utilization among older women [19] (Manyeh et al. 2020).
Barriers to FANC utilization: Barriers to FANC utilization at Chiga Health Centre are multifaceted and interrelated. Consistent with prior studies in Kenya and Ghana, inadequate awareness significantly impedes early and adequate ANC attendance (Manyeh et al. 2020) [19]. This aligns with recent global evidence. A systematic review by Simkhada et al. (2023) highlights that women’s knowledge about pregnancy risks and ANC benefits remains a primary determinant of timely ANC uptake in Low-and Middle-Income Countries (LMICs). Similarly, a 2022 study from Tanzania found targeted health education interventions significantly improved first-trimester ANC attendance (Mosha et al. 2022). This underscores the persistent challenge of educational gaps despite broad awareness campaigns. Health system factors, notably long waiting times and provider attitude, negatively impact service experience and repeat attendance [20]. Transportation and indirect economic costs remain significant challenges in rural settings despite policy provisions for free ANC services [3]. Studies from sub-Saharan Africa confirms these economic and logistical constraints limit ANC utilization (Onyeaka et al. 2023). This echoes WHO’s 2016 warning on hidden costs affecting health service equity and suggests a need for integrated transport and social support solutions tailored to rural contexts [3]. Cultural beliefs also influence health-seeking behavior, underscoring the need for culturally sensitive community engagement [4]. A 2023 multi-country study involving Uganda and Nigeria (Adepoju et al. 2023) documented that perceived disrespect and provider fatigue reduced continued engagement with ANC services. A 2024 ethnographic study in Ghana by Mensah et al. highlights how traditional norms and community influencer beliefs can either facilitate or hinder ANC uptake. Building on Gourounti et al. [4], current evidence advocates for culturally sensitive, participatory approaches that involve family and community leaders to foster trust and acceptance (Mensah et al. 2024). The WHO’s latest frameworks on quality of maternal care emphasize respectful maternity care as critical to improving ANC retention [14]. Investment in training and system efficiency remains vital.
Conclusion
Utilization of FANC services at Chiga Health Centre is constrained by knowledge deficits, logistical barriers, cultural influences, and health worker attitudes. Multisectoral interventions targeting these barriers are necessary to improve ANC attendance rates and subsequently maternal and neonatal health outcomes in Kisumu East Sub County.
Recommendations
• Implement community-based education programs to improve knowledge on FANC schedules and benefits.
• Introduce appointment systems to reduce waiting times.
• Develop transport support schemes or subsidies for pregnant women.
• Conduct regular training and supportive supervision aimed at enhancing healthcare provider-client interactions.
• Engage traditional leaders in maternal health promotion to address cultural barriers.
Declarations
Acknowledgment: We thank the staff of Chiga Health Centre and the participating women for their cooperation. Appreciation is extended to the Kisumu East Sub County for their oversight.
Ethical approval: This study was approved by Jaramogi Oginga Odinga Ethical Review Board Confidentiality was observed throughout the study period.
Competing interest: Authors have no competing interest.
Consent to participate: Informed consent was obtained from all participants involved in the study.
Authors’ contributions: R.Y Conceptualization and writing – original draft, R.Y, E.A & C.O Methodology, data curation formal analysis. N.C Supervision and writing-review and editing.
References
- Ahmed R, Kumar S, Lee J. Enhancing survey participation among older adults: challenges and strategies. J Popul Stud. 2021; 14: 210–225.
- Adewuyi EO, Adefemi K. Factors influencing antenatal care utilization among pregnant women: a systematic review. Matern Health J. 2022; 18: 45–59.
- Brown M, Williams T. Family formation and early adulthood: trends and implications. Sociol Rev. 2020; 68: 567–583.
- Chikumbu K, Dzwairo B, Mazonde I. Sociocultural barriers to antenatal care attendance in rural settings. Glob Health Action. 2021; 14: 193–204.
- Ditekemena J, Koole O, Engmann C, Matendo R, Tshefu A, Ryder R, et al. Male partner involvement in antenatal care and prevention of mother-to-child transmission of HIV. PLoS One. 2020; 15: e0236833.
- Garcia L, Thompson H. Marital patterns and social change: divorce and singlehood in the 21st century. J Soc Sci. 2023; 29: 34–50.
- Gourounti K, Anagnostopoulos F, Sandall J. Barriers and facilitators influencing pregnant women and health professionals in care. Midwifery. 2021; 90: 102847.
- Kabir MM, Chaudhury S, Begum T. Gender dynamics and maternal health care-seeking behavior in South Asia. Soc Sci Med. 2022; 294: 114682.
- Kassa GM, Arowojolu AO, Odukogbe AA, Yalew AW. Factors associated with utilization of antenatal care services in low- and middle-income countries. Reprod Health. 2020; 17: 1–16.
- Kruk ME, Gage AD, Arsenault C, Jordan K, Leslie HH, Roder-DeWan S, et al. High-quality health systems in the SDG era. Lancet Glob Health. 2018; 6: e1196–e1252.
- Johnson P, Smith R, Doe K. Demographic characteristics influencing survey responses in young adults. Res Methodol Q. 2022; 18: 142–157.
- Mbuthia EW, Mutea NJ, Manna AN. Impact of parity on antenatal care attendance in Kenya. BMC Pregnancy Childbirth. 2021; 21: 653.
- Nguyen T, Patel S. Marriage trends in developing countries: a demographic analysis. Int J Sociol. 2021; 55: 23–39.
- Ngatia PN, Onsongo JK, Onyango R. Determinants of utilization of focused antenatal care services in Kenya. BMC Health Serv Res. 2021; 21: 576.
- Smith J, Lee A. Young adults and social engagement: a demographic perspective. Youth Stud J. 2021; 12: 101–115.
- Tesfaye G, Molla G. Barriers to maternal health care access: influence of partner approval in Ethiopia. J Public Health. 2021; 43: 463–472.
- World Health Organization. WHO recommendations on antenatal care for a positive pregnancy experience. Geneva: WHO. 2016.
- World Health Organization. WHO recommendations on antenatal care for a positive pregnancy experience. Geneva: WHO. 2023.
- Yaya S, Ghose B. Global inequality in maternal health care service utilization. Health Equity. 2019; 3: 145–154.
- Kenya National Bureau of Statistics. Economic survey 2025. Nairobi: KNBS. 2025.