
Research ArticleOpen Access, Volume 4 Issue 1
Utility of polygenic risk scores and pharmacogenetic testing for cardiovascular risk management
Morcillo Serra César1*; Espinar Vicario Iñigo2; Canepa Leite Juan Pablo3; Martí Sánchez David2; Ortega Marcos Javier4; Jiménez Mena Manuel4; Zamorano Gómez José Luis5; Gutiérrez Gabriel Sonia6; Tomás Martínez José Francisco7; Suela Rubio Javier8
1Department of Internal Medicine, Sanitas Cima Hospital and Sanitas Medical Direction, Barcelona, Spain.
2Department of Cardiology, Sanitas Virgen del Mar Hospital, Madrid, Spain.
3Department of Cardiology, Sanitas Cima Hospital, Barcelona, Spain.
4Department of Cardiology, Sanitas La Moraleja Hospital, Madrid, Spain.
5Department of Cardiology, Sanitas La Zarzuela Hospital, Madrid, Spain.
6Research and Innovation Foundation, Sanitas Hospitals, Madrid, Spain.
7Department of Hematology, Sanitas Blua Valdebebas, Sanitas La Moraleja and Virgen del Mar Hospital, Madrid, Spain.
8Genetics Laboratory, Sanitas Hospitals, Madrid, Spain.
*Corresponding author: Morcillo Serra César
Department of Internal Medicine, Sanitas Cima Hospital and Sanitas Medical Direction, Ribera del Loira, 52, Madrid, Spain.
Email: cmorcillo@sanitas.es
Received : Jan 05, 2026 Accepted : Feb 26, 2026 Published : Mar 05, 2026
Epidemiology & Public Health - www.jpublichealth.org
Copyright: Morcillo Serra C © All rights are reserved
Citation: Morcillo Serra C, Espinar Vicario I, Canepa Leite JP, Martí Sánchez D, Ortega Marcos J, et al. Utility of polygenic risk scores and pharmacogenetic testing for cardiovascular risk management. Epidemiol Public Health. 2026; 4(1): 1093.
Abstract
Background: Polygenic Risk Scores (PRS) may aid in risk prediction and facilitate earlier interventions for primary prevention. Pharmacogenetic testing has the potential to optimize cardiovascular pharmacotherapy. This study aimed to evaluate the utility of PRS by comparing its results with the SCORE2 risk prediction algorithm and cardiovascular pharmacogenetic testing.
Methods: Cardiovascular risk was assessed using the SCORE2 chart. Patients were classified as having low (<99th percentile, Z-score <2) or high (≥99th percentile, Z-score ≥2) genetic risk based on PRS. The net reclassification risk and treatment changes influenced by pharmacogenetic testing were also evaluated.
Results: A total of 120 patients (mean age: 53.3 years; 66% male) were included. According to SCORE2, 68% were classified as low-moderate risk, 28% as high risk, and 4% as very high risk. Based on PRS, 31 (26% [18-33.7; 95% CI]) of low-moderate risk patients were reclassified as high risk. Treatment modifications occurred in 15 patients (12.5%), with 12 patients (10%) starting statins due to reclassification and 5 patients (4.2%) due to pharmacogenetic findings.
Discussion and conclusion: PRS reclassified 26% of patients assessed using the SCORE2 chart, enabling more patients to qualify for preventative treatment. Genetic testing influenced treatment decisions in 12.5% of patients. PRS and pharmacogenetic testing hold significant potential to enhance cardiovascular risk prediction and therapy optimization.
Keywords: Polygenic risk scores; Pharmacogenetic testing; Cardiovascular risk; Genetic risk.
Abbreviations: PRS: Polygenic Risk Score; CVD: Cardiovascular disease; CAD: Coronary Artery Disease; GWAS: Genome-Wide association Studies; ESC: European Society of Cardiology; HDL-C: High-Density Lipoprotein cholesterol; LDL-C: Low Density Lipoprotein Cholesterol; SNPs: Single Nucleotide Polymorphisms; CNVs: Copy Number Variations.
Introduction
The goal of population-level screening is to identify individu als at elevated disease risk who could benefit from timely in terventions. Cardiovascular Disease (CVD) screening poses chal lenges as approximately half of first coronary events, including sudden deaths, occur in asymptomatic individuals [1]. Ten-year CVD risk stratification is a crucial initial tool that guides clini cal evaluation and preventative measures in asymptomatic pa tients [2]. For high-risk individuals identified through SCORE2 charts, aggressive therapeutic interventions, such as primary prevention strategies, are recommended [3,4]. These strate gies can slow disease progression through lifestyle changes and pharmacological treatments.
However, intermediate-risk individuals require further evalu ation, as their true risk may be higher or lower depending on additional factors such as coronary artery calcium scoring [5,6]. The emergence of Genome-Wide Association Studies (GWAS) has enabled the development of PRS, which aggregate the small effects of millions of genetic variants across the genome to esti mate individual disease risk. PRS provide cost-effective, person alized enhancement of primary prevention [7], complementing traditional clinical tools such as SCORE2 [8].
Despite the lack of official guidelines for integrating PRS into clinical practice, evidence suggests that PRS could soon become a valuable tool for stratifying CVD risk and guiding treatment decisions [9]. For example, PRS combined with existing clinical models has demonstrated improved predictive performance in coronary artery disease (CAD) [10-13]. Furthermore, PRS guided lipid-lowering treatments for intermediate-risk patients have shown promise in reducing CVD events [14]. Although the 2021 European Society of Cardiology (ESC) guidelines acknowl edge the potential of PRS, further validation is required before its widespread clinical application [2]. Drugs with pharmacoge nomic evidence are common, yet they are only occasionally used, highlighting critical gaps that hinder precision medicine from becoming the standard of care [15].
This study aimed to assess the utility of PRS and pharmacoge netic testing in cardiovascular risk stratification and treatment by comparing the results of SCORE2 charts with PRS outcomes.
Materials & methods
Study design and participants
This quasi-experimental, cross-sectional study included 120 consecutive outpatients attending four Sanitas hospital cardi ology departments in Spain between July 2022 and December 2023, irrespective of referral type. Exclusion criteria included prior CVD diagnosis, diabetes mellitus, and age outside the range of 40-70 years. Based on literature analysis, a sample of 120 participants was selected with a predominance of low moderate and high CVD risks, to optimize the statistical power for evaluating the utility of PRS. Ethical approval was granted by the local ethics committee, and all participants provided written informed consent.
Data collection and measurements
During outpatient visits, patient history, physical examina tion findings, and fasting blood samples were collected to as sess cardiovascular risk factors. Analyzed variables included age, sex, obesity (BMI>30), smoking habits, hypertension (≥3 readings >140/90 mmHg), hypercholesterolemia (≥2 measure ments >250 mg/dL), and diabetes mellitus (fasting glucose ≥126 mg/dL or HbA1c ≥6.5%). Lipid profiles (total cholesterol, triglyc erides, HDL-C, LDL-C) were determined using enzymatic assays, and echocardiograms and stress tests were conducted.
Cardiovascular risk was calculated using SCORE2 tables for low-risk European populations, estimating 10-year fatal and non-fatal CVD event risks. Patients were categorized into low moderate, high and very high-risk groups [3].
A blood sample for genetic testing was collected at hospital centers, transported to the genetics laboratory, and analyzed. Genotyping was performed using array technology (Affymetrix PMDA - Custom Mee with 824.679 SNPs), and a cardiovascular PRS based on 6.6 million genetic variants was developed using the LDPred algorithm in individuals of European ancestry from the UK Biobank [16]. Reports detailing PRS and pharmacoge nomic data were uploaded to electronic health records. Phar macogenomic analyses included relevant genes influencing CVD treatment with real time PCR for the calculation of CYP2D6 CNVs.
Statistical analysis
Baseline characteristics were described using frequencies/ percentages for categorical variables. Concordance between SCORE2 and PRS risk classifications was evaluated using the kappa index. Statistical analyses were conducted using SPSS for Windows.
Results
Among the 120 participants (mean age: 53 years; 34% wom en), the SCORE2 algorithm categorized 68.3% as low-moderate risk, 28.3% as high risk, and 3.4% as very high risk. PRS analysis identified 72 patients (60%) as low-risk and 48 (40%) as high-risk (PRS score >3). Based on PRS, 31 (25.8% [18 to 33.7 with 95% confidence interval]) patients initially classified as low-mod erate risk by SCORE2 were reclassified as high-risk. Treatment modifications were observed in 15 patients (12.5%), including statin initiation in 12 patients (10%) following PRS reclassifi cation. For the remaining 16 patients reclassified as high risk, only lifestyle changes were recommended. Treatment changes were observed in 5 patients (4.2%) based on pharmacogenomic data. Specifically, the treatments most frequently changed by patients, in descending order, were statins, aspirin, angiotensin II antagonists, diuretics, beta-blockers, empagliflozin, amioda rone, and novel oral anticoagulants. All patients with treatment changes showed good pharmacological tolerance. For the 21 patients at high or very high risk according to SCORE2 but with a low-risk PRS, at the discretion of their cardiologists, treatment was not de-escalated.
Relevant cardiovascular risk factors and echocardiographic and stress test findings are shown in (Table 1).
(Figure 1) shows the correlation between cardiovascular risk by PRS and SCORE2. The kappa index between SCORE2 and PRS is 0.25, indicating low concordance.
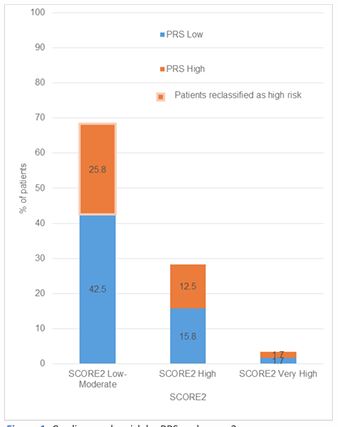
Table 1: Clinical characteristics of patients.
| Clinical characteristics of patients (120) | Value |
|---|---|
| Males | 79(66%) |
| Age | 53(51.9-54.7) |
| BMI >30 | 13(11%) |
| Smoking | 23(19%) |
| Hypertension | 42(35%) |
| Hypercholesterolemia | 74(62%) |
| Hypertriglyceridemia | 22(18%) |
| Positive Stress Test | 3(2.5%) |
| Echocardiogram with LVH | 1(1%) |
| Score 2 Low-Moderate Risk | 82(68%) |
| Score 2 High Risk | 34(28%) |
| Score 2 Very High Risk | 4(4%) |
Discussion
Our study demonstrates that the measurement of PRS re classified 26% of patients, initially evaluated using the SCORE2 chart, as high risk. This significant reclassification aligns with findings from Marston et al. who reported similar results in their study of 330,201 patients from the UK Biobank. In their analysis, CAD PRS effectively identified patients with borderline and intermediate clinical risk who would benefit from statin therapy. Specifically, when CAD PRS was added to the clinical CVD risk score in individuals younger than 50 years, 20% of those at borderline risk were reclassified into the intermediate risk group, warranting initiation of statin therapy. Conversely, 20% of patients with borderline or intermediate risk were re classified as low risk, thus eliminating the need for unnecessary treatment [17].
In our sample, 21(17%) patients with a SCORE2 of high or very high risk were reclassified to low risk according to the PRS result, which could have avoided unnecessary therapy. Con versely, 31(26%) patients with a SCORE2 of low risk were reclas sified to high risk according to the PRS, who would benefit from specific therapy. This reclassification highlights the potential of PRS to refine risk stratification and guide more personalized treatment decisions.
Another study, also using UK Biobank data, demonstrated that absolute CVD risk, determined through a clinical risk score, and relative genetic risk, determined by a PRS, provide inde pendent and complementary information. When these compo nents were combined into a simple multiplicative model, the precision of predicting incident CVD was significantly improved. This model reclassified 9.55% of intermediate-risk patients into the high-risk group, increasing the number of individuals in this category by 56.6% [15]. This finding underscores the value of integrating genetic risk with traditional clinical assessments to enhance predictive accuracy.
Although integrated risk tools that combine clinical scores with PRS have been shown to improve risk reclassification across multiple ethnicities and ancestries [18], the high percentage of reclassification observed in some studies like ours contrasts with others, which report rates between 2.5% and 8.7% [19]. Approximately 10% of incident CAD cases are misclassified as low risk by traditional risk calculators and are correctly reclassi fied as high risk using PRS [20]. This discrepancy suggests that PRS may offer a more precise risk assessment, particularly for individuals who fall into intermediate-risk categories.
PRS are based on inherited genetic variations, established at conception, and can thus be used early in life to guide life style modifications. In contrast, pooled cohort equations have only been validated for individuals aged 40 years and older. PRS also offer the advantage of estimating lifetime risk trajectories, rather than focusing on 5- or 10-year windows as most clini cal risk scores do. Since genetic risk is constant throughout life, PRS can be particularly valuable for younger individuals who have not yet developed clinical risk factors, such as hyperten sion or dyslipidemia, which are heavily influenced by lifestyle. Consequently, PRS could facilitate earlier interventions aimed at primary prevention [21]. For this reason, some authors rec ommend screening for PRS at birth or during childhood.
PRS information has the potential to motivate risk-reducing health behaviors, such as initiating medication, undergoing screening, or making lifestyle changes [22]. Emerging evidence highlights the positive behavioral impact of CAD PRS informa tion. Studies on the disclosure of CAD PRS results have shown increased perception of personal control, heightened infor mation-seeking behaviors [23], and the adoption of favorable health practices [24]. Moreover, shared decision-making in re sponse to PRS findings has resulted in more frequent statin pre scriptions [25]. Cross-sectional studies suggest that a favorable lifestyle can mitigate the increased risk associated with a high CAD PRS [26]. For example, individuals with a high PRS can re duce their lifetime risk of CAD by up to 50% through adherence to recommended lifestyle modifications [27].
In addition, elevated genetic risk is associated with earlier disease onset, even in the absence of traditional risk factors. Thus, PRS have the potential to enhance the accuracy of early and targeted primary prevention, particularly for chronic dis eases that develop over decades.
While most evidence suggests that combining PRS with non genetic risk factors maximizes clinical utility, PRS alone may be sufficient for individuals with extremely high scores. For in stance, individuals in the top 8% of the CAD PRS distribution have a risk comparable to that of individuals with a monogenic familial hypercholesterolemia mutation [28]. Based on equiva lent risk principles, it can be argued that individuals with PRS based risk levels similar to monogenic risks should qualify for comparable preventative therapies. While CAD PRS enhances risk stratification for future CVD, individuals with both high clini cal risk factors and elevated CAD PRS derive greater benefit (i.e., greater risk reduction) from statin therapy than those at lower PRS [29,30]. Furthermore, among patients with acute coronary syndrome and elevated lipid levels who received optimized statin therapy, a high CAD PRS was associated with a higher risk of recurrent cardiovascular events. These patients also experi enced greater risk reduction when treated with PCSK9 inhibi tors [31,32].
In our study, 12.5% of patients modified their treatment based on genetic testing results, either due to the PRS findings or pharmacogenomics, with good pharmacological tolerance. Pharmacogenomics holds the potential to optimize cardiovas cular pharmacotherapy and improve outcomes for patients with cardiovascular disease. Robust evidence supports genetic associations with drug dosage requirements and the risk of adverse effects [33]. The drugs with the strongest pharma cogenomic evidence include warfarin, clopidogrel, and statins, with accumulating data on genetic contributions to β-blocker response. Current guidelines recommend the use of pharmaco genetic testing to optimize warfarin dosing, select appropriate antiplatelet therapy after percutaneous coronary intervention, and predict the risk of statin-induced myopathy [34].
Limitations
This study should be interpreted with caution due to certain limitations, such as the small sample size, and challenges asso ciated with the deployment of PRS. Patients or physicians may misunderstand the uncertainties inherent in PRS-based risk estimates. Effective and clear risk communication by trained professionals is essential to minimize potential psychosocial ef fects. Additionally, individuals of non-European ancestry may receive inaccurate risk estimates due to the underrepresenta tion of these populations in large prospective genomic cohorts, potentially exacerbating healthcare disparities [35]. Further more, despite the demonstrated usefulness of PRS as a prog nostic tool in Anglo-Saxon populations, its implications in other settings remain unclear. Mediterranean countries, for instance, have a lower baseline risk of CVD, and it is necessary to evalu ate the prognostic value of elevated PRS in these populations. Studies are needed to assess the predictive capacity of PRS in quantifying coronary events and to evaluate the utility of pre ventive pharmacological interventions based on PRS findings in these regions.
Conclusion
Measurement of PRS reclassified 26% of patients as high risk when evaluated using the SCORE2 chart, potentially making more patients eligible for preventative treatment. Additionally, 12.5% of patients modified their treatment based on genetic testing, with good pharmacological tolerance. PRS and phar macogenetic testing hold significant promise for personalized medicine, optimizing cardiovascular risk prediction and phar macotherapy.
Declarations
Ethics approval: This study was approved by the Comité de Ética de la Investigación con Medicamentos (CEIm): Hospital Universitario La Princesa (registration no. 4953, approval 08-09 22, acta CEIm 16/22). All participants provided informed con sent before taking part in the study.
Conflicts of interest: The authors declare no conflicts of in terest.
Funding sources: This study did not receive any specific funding.
References
- Davies MJ. Anatomic features of victims of sudden death. Coronary artery pathology. Circulation. 1992; 85: 19–24.
- Visseren FLJ, Mach F, Smulders YM, et al; ESC Scientific Document Group. 2021 ESC guidelines on cardiovascular disease prevention in clinical practice. Eur Heart J. 2021; 42: 3227–3337.
- SCORE2 Working Group, ESC Cardiovascular Risk Collaboration. SCORE2 risk prediction algorithms: new models to estimate 10-year risk of cardiovascular disease in Europe. Eur Heart J. 2021; 42: 2439–2454.
- Wood D, de Backer G, Faergeman O, et al. Prevention of coronary heart disease in clinical practice: recommendations of the second joint task force of European and other societies on coronary prevention. Atherosclerosis. 1998; 140: 199–270.
- Yeboah J, McClelland RL, Polonsky TS, et al. Comparison of novel risk markers for improvement in cardiovascular risk assessment in intermediate-risk individuals. JAMA. 2012; 308: 788–795.
- Morcillo C, Valderas JM, Roca JM, et al. Computed tomographic measurement of coronary artery calcification in the assessment of cardiovascular risk: a descriptive study. Rev Esp Cardiol. 2007; 60: 268–275.
- Polygenic Risk Score Task Force of the International Common Disease Alliance. Responsible use of polygenic risk scores in the clinic: potential benefits, risks and gaps. Nat Med. 2021; 27: 1876–1884.
- Torkamani A, Wineinger NE, Topol EJ. The personal and clinical utility of polygenic risk scores. Nat Rev Genet. 2018; 19: 581–590.
- Elliott J, Bodinier B, Bond TA, et al. Predictive accuracy of a polygenic risk score-enhanced prediction model vs a clinical risk score for coronary artery disease. JAMA. 2020; 323: 636–645.
- Ganna A, Magnusson PKE, Pedersen NL, et al. Multilocus genetic risk scores for coronary heart disease prediction. Arter Thromb Vasc Biol. 2013; 33: 2267–2272.
- Abraham G, Havulinna AS, Bhalala OG, et al. Genomic prediction of coronary heart disease. Eur Heart J. 2016; 37: 3267–3278.
- Tada H, Melander O, Louie JZ, et al. Risk prediction by genetic risk scores for coronary heart disease is independent of self-reported family history. Eur Heart J. 2016; 37: 561–567.
- Inouye M, Abraham G, Nelson CP, et al. Genomic risk prediction of coronary artery disease in 480,000 adults: implications for primary prevention. J Am Coll Cardiol. 2018; 72: 1883–1893.
- Sun L, Pennells L, Kaptoge S, et al. Polygenic risk scores in cardiovascular risk prediction: a cohort study and modelling analyses. PLoS Med. 2021; 18: e1003498.
- Ronquillo JG, Lester WT. Pharmacogenomic testing and prescribing patterns for patients with cancer in a large national precision medicine cohort. J Med Genet. 2023; 60: 81–83.
- Li L, Pang S, Starnecker F, et al. Integration of a polygenic score into guideline-recommended prediction of cardiovascular disease. Eur Heart J. 2024; 45: 1843–1852.
- Marston NA, Pirruccello JP, Melloni GEM, et al. Predictive utility of a coronary artery disease polygenic risk score in primary prevention. JAMA Cardiol. 2023; 8: 130–137.
- O’Sullivan JW, Ashley EA, Elliott PM. Polygenic risk scores for the prediction of cardiometabolic disease. Eur Heart J. 2023; 44: 89–99.
- Weale ME, Riveros-McKay F, Selzam S, et al. Validation of an integrated risk tool, including polygenic risk score, for atherosclerotic cardiovascular disease in multiple ethnicities and ancestries. Am J Cardiol. 2021; 148: 157–164.
- Riveros-McKay F, Weale M, Moore R, et al. An integrated polygenic tool substantially enhances coronary artery disease prediction. Circ Genom Precis Med. 2021; 14: e003304.
- Hadley TD, Agha AM, Ballantyne CM. How do we incorporate polygenic risk scores in cardiovascular disease risk assessment and management? Curr Atheroscler Rep. 2021; 23: 28.
- McBride CM, Koehly LM, Sanderson SC, et al. The behavioral response to personalized genetic information: will genetic risk profiles motivate individuals and families to choose more healthful behaviors? Annu Rev Public Health. 2010; 31: 89–103.
- Brown SN, Jouni H, Marroush TS, et al. Effect of disclosing genetic risk for coronary heart disease on information seeking and sharing: the MI-GENES study. Circ Cardiovasc Genet. 2017; 10: e001613.
- Widén E, Junna N, Ruotsalainen S, et al. Communicating polygenic and non-genetic risk for atherosclerotic cardiovascular disease: an observational follow-up study. medRxiv. 2020.
- Kullo IJ, Jouni H, Austin EE, et al. Incorporating a genetic risk score into coronary heart disease risk estimates: effect on low-density lipoprotein cholesterol levels. Circulation. 2016; 133: 1181–1188.
- Khera AV, Emdin CA, Drake I, et al. Genetic risk, adherence to a healthy lifestyle, and coronary disease. N Engl J Med. 2016; 375: 2349–2358.
- Hasbani NR, Ligthart S, Brown MR, et al. American Heart Association’s Life’s Simple 7, polygenic risk, and lifetime risk of coronary heart disease. Circulation. 2022; 145: 808–818.
- Khera AV, Chaffin M, Aragam KG, et al. Genome-wide polygenic scores for common diseases identify individuals with risk equivalent to monogenic mutations. Nat Genet. 2018; 50: 1219–1224.
- Mega JL, Stitziel NO, Smith JG, et al. Genetic risk, coronary heart disease events, and the clinical benefit of statin therapy. Lancet. 2015; 385: 2264–2271.
- Natarajan P, Young R, Stitziel NO, et al. Polygenic risk score identifies subgroup with higher burden of atherosclerosis and greater relative benefit from statin therapy. Circulation. 2017; 135: 2091–2101.
- Damask A, Steg PG, Schwartz GG, et al. Patients with high genome-wide polygenic risk scores for coronary artery disease may receive greater clinical benefit from alirocumab treatment in the ODYSSEY OUTCOMES trial. Circulation. 2020; 141: 624–636.
- Marston NA, Kamanu FK, Nordio F, et al. Predicting benefit from evolocumab therapy using a genetic risk score: results from the FOURIER trial. Circulation. 2020; 141: 616–623.
- Duarte JD, Cavallari LH. Pharmacogenetics to guide cardiovascular drug therapy. Nat Rev Cardiol. 2021; 18: 649–665.
- Cavallari LH, Mason DL. Cardiovascular pharmacogenomics: implications for patients with chronic kidney disease. Adv Chronic Kidney Dis. 2016; 23: 82–90.
- Babb de Villiers C, Kroese M, Moorthie S. Understanding polygenic models, their development and the potential application of polygenic scores in healthcare. J Med Genet. 2020; 57: 725–732.