
Research ArticleOpen Access, Volume 3 Issue 1
Assessment of haematocrit and serum ferritin levels of Calabar healthy adult residents
Grace Igebu1*; EA Asemota1; Olasehinde Olusanya2,3
1Department of Medical Laboratory Science, Faculty of Allied Medical Sciences, University of Calabar, Calabar, Nigeria.
2Institute of Biophysics, Chinese Academy of Sciences (CAS), University of Chinese Academy of Sciences, China.
3Department of Biochemistry, University of Benin, Nigeria.
*Corresponding author: Grace Igebu
Department of Medical Laboratory Science, Faculty of Allied Medical Sciences, University of Calabar, Calabar, Nigeria.
Email: grace_iigebu@yahoo.com
Received : Mar 12, 2025 Accepted : April 23, 2025 Published : Apr 30, 2025
Epidemiology & Public Health - www.jpublichealth.org
Copyright: Igebu GC © All rights are reserved
Citation: Igebu G, Asemota EA, Olusanya O. Assessment of haematocrit and serum ferritin levels of Calabar healthy adult residents. Epidemiol Public Health. 2025; 3(1): 1067.
Abstract
Understanding the relationship between Packed Cell Volume (PCV) and serum ferritin levels is essential for evaluating iron status and overall health, particularly in young adults in minority communities. This study assessed Packed Cell Volume (PCV) and serum ferritin levels among 84 Calabar residents (40 females, 44 males) aged 18-35. PCV was measured using the microhaematocrit method, and serum ferritin via Enzyme-Linked Immunoassay (ELISA). Males exhibited significantly higher mean PCV (0.47±0.07 L/L) and serum ferritin levels (89.31±90.7 ng/mL) than females (0.39±0.07 L/L, 47.00±91.5 ng/mL) with p-values of 0.000 and 0.037, respectively. By age group, no significant differences were observed in PCV or serum ferritin levels (p=0.823 and p=0.150, respectively). However, males consuming three meals per day had significantly higher PCV, serum ferritin, and Body Mass Index (BMI) (0.49±0.03 L/L, 165.9 107.9 ng/mL, 28.04±2.57 kg/m²) compared to those eating two meals daily (p=0.00, 0.03, and 0.00, respectively). Females eating three meals daily showed higher PCV (0.42±0.02 L/L) and serum ferritin (78.55±22.85 ng/mL), though differences in ferritin and BMI were not significant. A positive correlation between PCV and serum ferritin was found in both sexes (r=0.3209 in males, r=0.2782 in females), indicating a statistically significant relationship. The results suggest that female students have lower PCV and serum ferritin levels, likely due to menstrual blood loss and differing lifestyle factors. These findings highlight the need for targeted nutritional interventions to address gender-specific health disparities.
Keywords: Serum; PCV; Ferritin; Students; Feeding; BMI.
Introduction
Iron is an indispensable bioelement essential for various biological functions. It is distributed throughout the body, with approximately 3000 mg found in hemoglobin within red blood cells, 400 mg in myoglobin of muscle cells, 50 mg in cytochromes and iron-sulfur proteins in tissues, and 5 mg in transferrin of plasma and extracellular fluids. Furthermore, 100-1000 mg of iron is stored in ferritin and hemosiderin in organs such as the liver, spleen, and bone marrow [1,2]. Hemoglobin is crucial for oxygen transport from the lungs to tissues, while myoglobin, found in muscle cells, plays a role in storing and releasing oxygen [3]. Despite its vital role, free ionic iron is toxic and must be stored safely inside cells. To manage this, vertebrates have evolved protective mechanisms to bind iron across various tissue compartments [4,5].
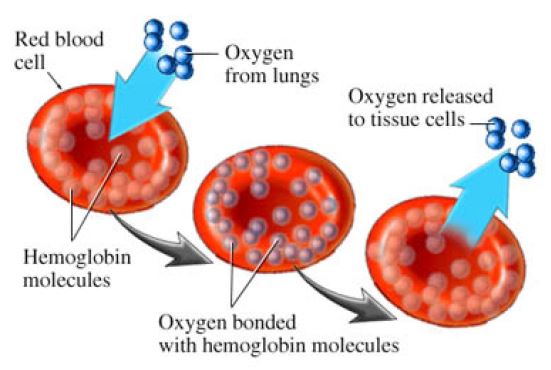
Hemoglobin is a protein complex containing iron, which plays a critical role in oxygen transport within the bloodstream. Hemoglobin molecules aggregate within red blood cells (erythrocytes), which are characterized by their distinctive biconcave, disc-like shape. Each hemoglobin molecule consists of four heme groups, each of which provides a binding site for one oxygen molecule. Consequently, a single hemoglobin molecule can bind a maximum of four oxygen molecules, representing its full oxygen-carrying capacity [6].
Dietary intake provides the body’s iron, with absorption influenced by diet composition, bioavailability, and physiological demand. A normal Western diet typically supplies around 15 mg of iron daily, of which 1 mg (5-10%) is absorbed into the bloodstream in healthy adults [7]. Ferritin, an intracellular protein, stores about 25% of the body’s iron and releases it when needed. In adult males, the average stored iron is 1000 mg (sufficient for about three years), while women typically store 300 mg (enough for six months) [8,9]. Ferritin not only buffers against iron deficiency but also protects against overload, functioning as a crucial regulator of iron homeostasis in humans. It is produced by all living organisms and is found in most tissues as a cytosolic protein, although small amounts circulate in the blood to act as an iron carrier [10].
Serum ferritin is an indirect marker of total body iron and is widely used in diagnosing iron deficiency anemia [11]. The Iron Disorder Institute’s Scientific and Medical Advisory Board recommends a serum ferritin range of 50-150 ng/ml for adults to ensure proper iron management [12]. Elevated serum ferritin levels are observed in conditions such as hemochromatosis, fatty liver disease, and iron overload syndromes, while reduced levels indicate iron deficiency [12].
Packed Cell Volume (PCV), also known as hematocrit, measures the proportion of red blood cells in blood and is a key indicator in diagnosing anemia and other blood disorders [13,14]. It forms part of a comprehensive blood count, alongside hemoglobin, white blood cell count, and platelet count [15]. Elevated PCV levels are associated with conditions like polycythemia vera, chronic obstructive pulmonary disease, and dehydration, while low PCV levels suggest anemia [16]. Previously, Okpokam et al. [17] demonstrated higher PCV and serum ferritin values in healthy controls compared to blood donors, reinforcing the relationship between iron status and blood parameters.
Despite extensive research on iron metabolism and its critical role in maintaining health, there is a notable gap in understanding how these processes vary across different demographic groups, particularly in minority communities such as those in Calabar. For example, Mgbekem et al. [18] investigated the food consumption patterns and nutritional status of People Living With HIV (PLWH) in Calabar, focusing on differences between those on Antiretroviral Therapy (ART), those not on treatment (NART), and a non-infected control group. Their study revealed that nutritional status, including BMI, was significantly lower in the NART group compared to others, linking food intake directly to health outcomes in PLWH. Similarly, Onyenweaku et al. [19,20] examined the contribution of cholesterol-containing foods, like eggs, to dietary cholesterol intake and their impact on serum lipid profiles in adults, concluding that dietary cholesterol did not significantly raise serum cholesterol levels in normocholesterolemic individuals. Inah et al. [21] explored the nutrient intake among pregnant women in Calabar, showing a significant prevalence of nutrient inadequacy, particularly concerning energy intake, which correlated with maternal age, educational level, and BMI. The studies share a common focus on dietary patterns and their health implications for different demographic groups in Calabar, Nigeria. Mgbekem et al. [18] linked food consumption to nutritional status in PLWH, while Onyenweaku et al. [20] focused on cholesterol and lipid profiles, and Inah et al. [21] emphasized nutrient inadequacies in pregnant women. Collectively, these studies underscore the importance of assessing nutritional intake and its broader health impacts, highlighting the need for specific dietary interventions tailored to vulnerable populations. However, no studies every focused on assessing haematocrit and serum ferritin levels in healthy adult residents of Calabar. Monitoring these biomarkers provides critical insights into iron status and overall health, complementing existing data on nutrition and health outcomes in the region. This would help identify potential deficiencies or imbalances that might not be captured solely by dietary assessments, thus addressing gaps in the current understanding of the population’s nutritional status. Additionally, most existing studies focus on populations in developed regions, often overlooking the unique socioeconomic, dietary, and health challenges faced by underserved groups. In Calabar, the prevalence of iron deficiency and related anemia remains underexplored, especially considering the potential influence of local dietary habits, genetic predispositions, and healthcare access. There is limited data on how these factors impact serum ferritin levels and Packed Cell Volume (PCV) in this population. Addressing this gap is essential for developing targeted interventions to improve iron status and overall health outcomes in minority communities.
Experimental methods and study participants
Participants: This study involved 84 students from the Calabar, including both male and female volunteers. Participants provided informed consent before completing a socio-demographic questionnaire (see Supplementary Material). Blood samples were collected for the determination of Packed Cell Volume (PCV) and serum ferritin levels. PCV was measured using the microhematocrit method, and serum ferritin was determined using an enzyme-linked immunosorbent assay (ELISA) kit (Monobind Inc., Lake Forest, CA, USA; Product Code: 2825-300).
Sample collection: Venous blood (5 mL) was drawn aseptically from the antecubital vein. Of this, 2 mL was placed in an EDTA tube for PCV analysis, and 3 mL was stored in a plain tube for serum ferritin assay. Samples were transported on ice to the laboratory.
Sample handling and storage: in the plain tube was allowed to clot, centrifuged at 3000 rpm for 5 minutes, and the serum was stored at -20°C for ferritin assay.
ELISA assay for serum ferritin: Samples were processed using a sequential immunoenzymometric assay. Monoclonal biotinylated antibodies reacted with the antigen in the serum, and the antigen-antibody complex bound to streptavidin-coated microwells. After incubation and washing, enzyme-labeled antibodies were added, followed by a colorimetric substrate for measurement via spectrophotometry at 450 nm.
Microhematocrit method for PCV: Anticoagulated blood was centrifuged at 12,000 g for 5 minutes in a capillary tube. The PCV was read using a microhematocrit reader.
Statistical analysis
Data were analyzed using Microsoft Excel to calculate means and standard deviations. Student’s t-test, ANOVA, and correlation analyses were used for statistical comparisons.
Results
The study evaluated Packed Cell Volume (PCV) and serum ferritin concentrations in a cohort of 84 young adults residing in Calabar, aged 18-35 years. Among the participants, 40 were female, and 44 were male. (Table 1) outlines the mean PCV and serum ferritin values stratified by gender. Males exhibited a mean PCV of 0.47±0.7 L/L and a mean serum ferritin level of 89.31± 90.7 ng/mL, whereas females displayed a mean PCV of 0.39±0.7 L/L and a mean serum ferritin concentration of 47.00±91.5 ng/mL. Statistical analysis revealed that these differences were highly significant, with p-values of 0.000 and 0.037, respectively.
(Table 2) presents the data stratified by age groups, revealing that 94% (n=79) of participants were aged between 18 and 29 years, while only 6% (n=5) were aged 30-35. For participants aged 18-23 years, the mean PCV was 0.427±0.05 L/L, with a corresponding serum ferritin value of 67.53±96.86 ng/mL. Those aged 24-29 years demonstrated a mean PCV of 0.434±0.05 L/L and serum ferritin of 55.13±40.01 ng/mL. The older age group (30-35 years) exhibited a mean PCV of 0.438±0.04 L/L and serum ferritin of 144.54±166.28 ng/mL. No significant differences were observed between these groups (p=0.823 for PCV and p=0.15 for serum ferritin).
Table 1: Packed cell volume and serum ferritin values based on gender.
| Parameters | Male n=44 | Female n=40 | P-value |
|---|---|---|---|
| x̄±SD | x̄±SD | ||
| PCV (l/l) | 0.47±0.7 | 0.39±0.7* | 0 |
| Serum ferritin (ng/ml) | 89.31±90.7 | 47.00±91.5* | 0.037 |
*Means significantly different when compared to corresponding gender (P<0.05).
Table 2: Packed cell volume and serum ferritin values based on age.
| Parameters | Age: 18-23 | Age: 24-29 | Age: 30-35 | P-value |
|---|---|---|---|---|
| n=59, | n=20 | n=5 | ||
| x̄±SD | x̄±SD | x̄±SD | ||
| PCV (l/l) | 0.427±0.05 | 0.434±0.05 | 0.438±0.04 | 0.823 |
| Serum ferritin (ng/ml) | 67.53±96.86 | 55.13±40.01 | 144.54±166.28 | 0.15 |
Further analysis, displayed in (Table 3), examined PCV, serum ferritin, and Body Mass Index (BMI) by gender based on the frequency of meals consumed per day. Male students who consumed three meals daily had a mean PCV of 0.49±0.03 L/L, a serum ferritin level of 165.9±107.9 ng/mL, and a BMI of 28.04±2.57 kg/m². Comparatively, those who ate two meals per day exhibited significantly lower values: a mean PCV of 0.44±0.04 L/L, serum ferritin of 70.56±72.18 ng/mL, and a BMI of 23.39±2.65 kg/m² (p=0.00, p=0.03, and p=0.00, respectively). Female students showed similar trends; those consuming three meals had a mean PCV of 0.42±0.02 L/L, while those eating twice daily had a significantly lower mean PCV of 0.39±0.04 L/L (p=0.01). However, no significant differences were observed in serum ferritin and BMI values among females based on meal frequency (p=0.08 for serum ferritin and p=0.16 for BMI).
Table 3: Packed cell volume, serum ferritin and body mass index values based on frequency of feeding.
| Parameters | Males | Females | ||||
|---|---|---|---|---|---|---|
| 2/day n=35 | 3/day n=9 | P-value | 2/day n=31 | 3/day n=9 | P-value | |
| x̄±SD | x̄±SD | x̄±SD | x̄±SD | |||
| PCV (l/l) | 0.44±0.04 | 0.49±0.03* | 0 | 0.39±0.04 | 0.42±0.02* | 0.01 |
| SF (ng/ml) | 70.56±72.18 | 165.9±107.9* | 0.03 | 43.83±102.4 | 78.55±22.85 | 0.08 |
| BMI (kg/m3) | 23.39±2.65 | 28.04±2.57* | 0 | 23.41±4.15 | 25.46±3.51 | 0.16 |
*Means significantly different when compared to corresponding frequency of feeding (P<0.05).
(Table 4) details the impact of dietary choices on PCV, serum ferritin, and BMI in male students. Those who regularly consumed unripe plantain had a significantly higher mean PCV (0.46±0.03 L/L) compared to those who predominantly consumed red meat (0.44±0.05 L/L) or vegetables (0.41±0.03 L/L) (p=0.01). No significant differences were observed in serum ferritin or BMI values among these dietary groups (p=0.17 and p=0.39, respectively). Similarly, (Table 5) outlines the results for female students, with those consuming red meat exhibiting a significantly higher mean PCV (0.41±0.03 L/L) compared to those eating vegetables (0.40±0.04 L/L) and unripe plantain (0.39±0.03 L/L) (p=0.00). However, there were no significant differences in serum ferritin or BMI among these groups (p=0.41 and p=0.21, respectively).
Table 4: Packed cell volume, serum ferritin and body mass index values in male students based on consumption of different food types.
| Parameters | Unripe plantain | Red meat | Vegetable | P-value |
|---|---|---|---|---|
| n=20 | n=14 | n=10 | ||
| x̄±SD | x̄±SD | x̄±SD | ||
| PCV (l/l) | 0.46±0.03 | 0.44±0.05 | 0.41±0.03* | 0.01 |
| SF (ng/ml) | 108.63±90.02 | 89.87±114.63 | 42.25±25.49 | 0.17 |
| BMI (kg/m3) | 24.77±2.79 | 24.44±2.08 | 23.38±2.43 | 0.39 |
*Means significantly different when compared to other food types (P<0.05).
Table 5: Packed cell volume, serum ferritin and body mass index values in female students based on type of food.
| Parameters | Male | Female | ||||
|---|---|---|---|---|---|---|
| Offcampus | On campus | P-value | Offcampus | On campus | P-value | |
| n=24 | n=20 | n=19 | n=21 | |||
| x̄±SD | x̄±SD | x̄±SD | x̄±SD | |||
| PCV (l/l) | 0.48±0.03 | 0.43±0.04* | 0 | 0.42±0.02 | 0.39±0.03* | 0 |
| SF (ng/ml) | 127.43±106. 95 | 39.74±26. 33* | 0 | 79.17±126.3 | 21.53±16.79 | 0.06 |
| BMI (kg/m3) | 24.41±2.33 | 23.51±2.86 | 0.26 | 24.23±4.38 | 23.94±4.47 | 0.84 |
*Means significantly different when compared to other food types (P<0.05).
Table 6: Packed cell volume, serum ferritin and body mass index values based on geographical location.
| Parameters | Male | Female | ||||
|---|---|---|---|---|---|---|
| Offcampus | On campus | P-value | Offcampus | On campus | P-value | |
| n=24 | n=20 | n=19 | n=21 | |||
| x±SD | x±SD | x±SD | x±SD | |||
| PCV (l/l) | 0.48±0.03 | 0.43±0.04* | 0 | 0.42±0.02 | 0.39±0.03* | 0 |
| SF (ng/ml) | 127.43±106. 95 | 39.74±26. 33* | 0 | 79.17±126.3 | 21.53±16.79 | 0.06 |
| BMI (kg/m3) | 24.41±2.33 | 23.51±2.86 | 0.26 | 24.23±4.38 | 23.94±4.47 | 0.84 |
*Means significantly different when compared to geographical location (P<0.05).
The influence of geographical location (on-campus vs. off-campus residence) on PCV, serum ferritin, and BMI is presented in (Table 6). Male students residing off-campus had significantly higher mean PCV (0.48±0.03 L/L) and serum ferritin levels (127.43±106.95 ng/mL) compared to their on-campus counterparts (PCV: 0.43±0.04 L/L, serum ferritin: 39.74±26.33 ng/mL) (p=0.00 for both). BMI values, however, did not differ significantly between the two groups (p=0.26). Among female students, those living off-campus exhibited a significantly higher mean PCV (0.42±0.02 L/L) than those living on-campus (0.39±0.03 L/L) (p=0.00), though no significant differences were noted in serum ferritin or BMI (p=0.06 and p=0.84, respectively).
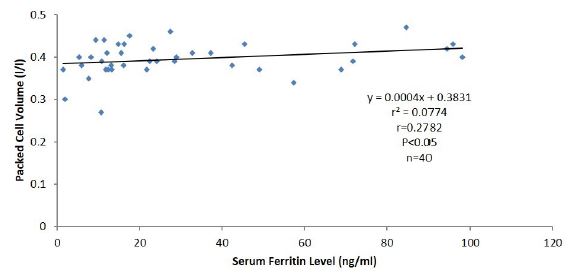
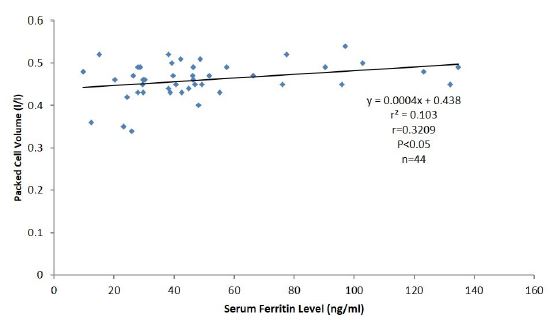
(Figure 2) illustrates the positive correlation between PCV and serum ferritin levels in female participants, with a correlation coefficient (r) of 0.2782, indicating statistical significance (p<0.05). Similarly, (Figure 3) depicts the positive correlation observed in male participants, with an r-value of 0.3209, also statistically significant (p<0.05).
These results suggest that serum ferritin concentration is positively associated with PCV in both male and female residents living in Calabar.
Discussion
Ferritin, a protein responsible for storing iron, exists in blood at very low concentrations, with only about 1% of plasma iron being stored in this form. Serum ferritin levels serve as a reliable biomarker for assessing the body’s total iron stores and are frequently used to screen for iron deficiency in various populations, including blood donors, individuals receiving regular blood transfusions, or those undergoing iron replacement therapy [1]. Clinicians utilize serum ferritin as a diagnostic indicator due to its strong correlation with the body’s iron reserve.
In this study, a statistically significant disparity in mean Packed Cell Volume (PCV) and serum ferritin levels was observed between male and female participants, with males exhibiting significantly higher values (p=0.000 and p=0.037, respectively). This observation aligns with established reference ranges as reported by Cheesbrough [22] and is consistent with findings from similar studies, such as those conducted among blood donors by Erhabor et al. [23]. Comparable results were also reported in Calabar when control participants were compared to blood donors [17]. The observed gender differences could be multifactorial, potentially influenced by variations in dietary intake, menstrual blood loss in females, hormonal influences, and physical activity levels in males. Additionally, iron deficiency disproportionately affects premenopausal women due to menstrual blood loss, as highlighted by Sant-Rayn Pasricha et al. which notes that iron deficiency is a leading contributor to the global burden of disease, particularly in premenopausal women, children, and low-income populations. Auerbach et al. further emphasize that while iron deficiency often leads to anemia, functional impairments can occur even in its absence, and its prevalence is exacerbated by inadequate iron supplementation. These findings suggest that gender-specific physiological factors, including menstrual blood loss and the differing approaches to iron supplementation, contribute significantly to the disparities observed.
The lack of significant variation in mean PCV and serum ferritin levels across different age groups (p>0.05) further indicates that these values remain within the normal adult reference range, as described by Cheesbrough [22]. The relatively small number of participants in certain age groups may have contributed to the lack of statistical significance in these comparisons. The influence of sample size should be considered in future investigations, as it may affect the statistical power and generalizability of the results.
The study also found that females who consumed three meals daily exhibited higher mean PCV, serum ferritin, and body mass index (BMI) values compared to those who ate twice a day. These results align with findings from a study conducted among female students at King Abdulaziz University in Saudi Arabia [24]. Additionally, research has shown that female participants who consumed red meat and vegetables less than twice weekly were at an increased risk of developing iron deficiency [25]. This study identified that 11.9% of the participants had low serum ferritin levels, a prevalence lower than the 20.6% reported among blood donors in Port Harcourt [26]. The discrepancy may be attributable to dietary factors, including lower consumption of iron-rich foods such as red meat, vegetables, and unripe plantains among the study population.
Furthermore, students residing off-campus had significantly higher PCV, serum ferritin, and BMI values compared to those living on-campus. This difference could be linked to socioeconomic factors, such as higher income or greater food allowances for off-campus students, which enable them to consume a more balanced and nutritious diet. Improved dietary quality and frequency of meals likely contribute to better overall health, as indicated by the higher hematological and anthropometric indices.
A positive and statistically significant correlation was observed between PCV and serum ferritin levels for both male and female students, with correlation coefficients of r=0.3209 and r=0.2782, respectively (p<0.05). This finding supports previous studies, such as that by Okpokam et al. [17], which reported a significant positive correlation between serum ferritin levels and PCV among 163 male blood donors. The relationship between these two parameters is biologically plausible, as iron is a critical component in erythropoiesis, the process by which red blood cells are produced. Adequate iron stores, reflected by serum ferritin levels, are essential for maintaining optimal PCV, thus underscoring the importance of iron in hematopoiesis.
It is worth reiterating that this study highlights the complex interplay between gender, diet, socioeconomic status, and iron metabolism, with significant implications for understanding how these factors influence hematological parameters. Future research should consider larger sample sizes and longitudinal designs to further elucidate these relationships and explore potential interventions aimed at improving iron status and overall health in populations at risk of deficiency.
Conclusion
The present study provides significant insights into the hematological profiles of Calabar adult residents, with a particular focus on Packed Cell Volume (PCV) and serum ferritin levels. The findings reveal that both PCV and serum ferritin values are notably lower among female residents, which may be attributed to the physiological demands of menstruation, compounded by insufficient dietary iron intake. Additionally, residents who consume fewer meals per day, specifically those consuming only two meals, demonstrate suboptimal iron status as reflected by reduced ferritin concentrations. This nutritional inadequacy is further exacerbated among both male and female residents residing on campus, likely due to limited access to diverse and nutrient-dense meals. These results underscore the impact of dietary habits, gender-specific physiological demands, and socioeconomic factors on iron metabolism and overall hematological health. The study highlights a critical need for targeted interventions to address the nutritional gaps and iron deficiency risk in this population, particularly among female residents who are at greater risk due to regular menstrual blood loss.
Recommendations
Given the findings of this study, several measures are imperative to mitigate the risk of iron deficiency and improve the hematological health of students at tertiary institutions:
1. Implementation of nutritional awareness and education programs: A broad nutritional awareness campaign should be developed and implemented, focusing particularly on female residents. This program should emphasize the importance of a balanced diet rich in iron, including sources such as red meat, leafy green vegetables, and fortified grains. Educational materials should also address the increased iron requirements during the menstrual cycle and the risks associated with inadequate iron intake.
2. Menstrual health and dietary support: Special attention should be given to female residents due to their higher susceptibility to iron deficiency caused by menstrual blood loss. Programs should advocate for iron-rich diets and supplementation when necessary, particularly for students who may have difficulty meeting their iron needs through diet alone. Collaborations with healthcare providers to offer individualized dietary counseling and iron supplementation, especially during peak menstrual periods, should be considered.
3. Dietary improvement initiatives: For students, university dining services should prioritize the availability of balanced meals with adequate portions of iron-rich foods. Meal plans should be designed to meet the nutritional needs of students, with particular emphasis on those residing on campus who may face financial or logistical challenges in accessing nutrient-dense foods. Ensuring that meals provided at on-campus dining facilities are both affordable and nutritionally adequate is critical to addressing the observed deficiencies.
4. Regular health and hematological screening: Routine screening of hematological parameters, including serum ferritin and PCV, should be instituted as part of health services offered to students. Regular monitoring would facilitate early identification of iron deficiency and anemia, allowing for timely intervention through dietary modification, supplementation, or further medical evaluation if necessary.
5. Collaboration with health services and policy makers: Tertiary institutions should collaborate with public health authorities and policymakers to develop strategies for addressing the nutritional challenges faced by residents and students. This may include subsidizing iron-rich foods for students or providing access to fortified food products. Engaging in interdisciplinary efforts to bridge the gap between health, nutrition, and education is essential for long-term improvements in student well-being.
6. By addressing these critical areas, it is possible to enhance the overall nutritional status and health outcomes of students, thus fostering a healthier academic environment conducive to optimal learning and performance. However, it worth mentioning that present study is limited by its cross-sectional design, which restricts the ability to establish causality between dietary habits, iron status, and hematological outcomes. In addition, the sample size and geographic focus on Calabar residents may limit the generalizability of the findings to broader populations, and potential confounding factors, such as the use of supplements or underlying health conditions, were not thoroughly addressed.
References
- Dacie JV, Lewis SM. Iron deficiency anaemia and iron overload. In: Practical Haematology. 11th ed. Churchill Livingstone. 2012: 176-9.
- Skalnaya MG, Skalny AV. Essential trace elements in human health: a physician’s view. Tomsk: Publishing House of Tomsk State University. 2018: 1-222.
- Cao M, Wang G, He H, Yue R, Zhao Y, Pan L, et al. Hemoglobin-based oxygen carriers: potential applications in solid organ preservation. Front Pharmacol. 2021; 12: 760215.
- Orino K, Lehman L, Tsuji Y, Ayaki H, Torti SV, Torti FM. Ferritin and the response to oxidative stress. Biochem J. 2001; 357: 241-7.
- Venkataramani V. Iron homeostasis and metabolism: two sides of a coin. In: Ferroptosis: Mechanism and Diseases. 2021: 25-40.
- Oto B. Respiration and hemoglobin. EMS basics. Available from: https://emsbasics.com/2011/08/03/respiration-and-hemoglobin/
- Briguglio M, Hrelia S, Malaguti M, Lombardi G, Riso P, Porrini M, et al. The central role of iron in human nutrition: from folk to contemporary medicine. Nutrients. 2020; 12: 1761.
- Estaintot BL, Santambrogio P, Granier T, et al. Crystal structure and biochemical properties of the human mitochondrial ferritin and its mutant Ser144Ala. J Mol Biol. 2004; 340: 277-93.
- Leong WI, Lönnerdal B. Iron nutrition. In: Iron physiology and pathophysiology in humans. 2012: 81-99.
- Frazer DM, Anderson GJ. The regulation of iron transport. Biofactors. 2014; 40: 206-14.
- Conrad ME, Umbreit JN. Disorders of iron metabolism. N Engl J Med. 2000; 342: 1293-4.
- Sidell B, Kristin OB. When bad things happen to good fish: the loss of hemoglobin and myoglobin expression in Antarctic ice fishes. J Exp Biol. 2006; 209: 1791-802.
- Baker FJ, Silverton RE, Pallister CJ. The full blood count. In: Introduction to Medical Laboratory Science. 7th ed. Bounty Press; 2009: 360-1.
- Gajbhiye S, Aate J. Blood report analysis: a review. Trop J Pharm Life Sci. 2023; 10: 63-79.
- Purves WK, David S, Gordan H, Orians H, Craig H. Life: The Science of Biology. 7th ed. Sinauer Associates. 2004: 954.
- Goodnough LT, Schrier SL. Evaluation and management of anemia in the elderly. Am J Hematol. 2014; 89: 88-96.
- Okpokam DC, Emeribe AO, Akpotuzor JO. Frequency of blood donation and iron stores of blood donors in Calabar. Int J Biomed Lab Sci. 2011; 1: 40-3.
- Mgbekem MA, Atangwho IJ, Duke E, Ukam N, Ojong M, John ME, et al. Food consumption patterns and nutritional status of People living with HIV in Calabar. Pak J Nutr. 2015; 14: 726-34.
- Onyenweaku EO, Oko GE, Fila WA. Snack consumption pattern of adults in the University of Calabar and its health implications. Eur J Nutr. Food Saf. 2019; 10: 43-49.
- Onyenweaku EO, Ene-Obong HN, Oko GE, Williams IO. Contribution of eggs and other cholesterol-containing foods to total dietary cholesterol intake, and their influence on serum lipid profile of adults in Calabar, Nigeria. European Journal of Nutrition & Food Safety. 2019; 9: 329-340.
- Inah GM, Iyam M, Mgban E. Food and Nutrient Intake of Pregnant Women of the out-Patient Department of General Hospital, Calabar, Nigeria. Global Journal of Pure and Applied Sciences. 2012; 18: 213-220.
- Cheesbrough M. Haematological tests. In: Laboratory practice in tropical countries. 2nd ed. Cambridge University Press. 2010: 312-3.
- Erhabor O, Imrana S, Buhari HA, Abdulrahaman Y, et al. Iron deficiency among blood donors in Sokoto, Northwestern Nigeria. Open J Blood Dis. 2014; 4: 33-42.
- Al-Sayes F, Gari M, Qusti S, Bagatian N, Abuzenadah A. Prevalence of iron deficiency and iron deficiency anaemia among females at university stage. J Med Lab Diagn. 2010; 2: 5-11.
- Al-Quaiz JM. Iron deficiency anaemia: A study of risk factors. Saudi Med J. 2001; 22: 490-6.
- Zaccheaus AJ, Baribe FK. Anaemia, iron deficiency and iron deficiency anaemia among blood donors in Port Harcourt. Blood Transfus. 2010; 8: 113-7.