
Research ArticleOpen Access, Volume 1 Issue 3
Perceived Experience and Management of Covid-19 in Southeastern Nigeria
Uchechukwumadukaku Chukwuocha1 ; George Tamunowengifiri Charles1 ; David Chinaecherem Innocent1*; Joshua Chisom Ogboeze1 ; Rejoicing Chijindum Innocent2 ; Chiagoziem Ogazirilem Emerole1 ; Ramesh Kumar3 ; Ali A Rabaan4,5,6; John Chigozie Ekenze7 ; Ihuoma Chimdimma Dike1
1Department of Public Health, Federal University of Technology Owerri, Imo State Nigeria.
2Department of Pharmacy, Enugu State University of Science and Technology, Enugu State, Nigeria.
3Health Service Academy, Islambad, Pakistan.
4Molecular Diagnostic Laboratory, Johns Hopkins Aramco Healthcare, Dhahran 31311, Saudi Arabia.
5College of Medicine, Alfaisal University, Riyadh 11533, Saudi Arabia.
6Department of Public Health and Nutrition, University of Haripur, Haripur 22610, Pakistan.
7Department of Optometry, Imo State University, Owerri, Imo State, Nigeria.
*Corresponding author: David Chinaecherem Innocent
Department of Public Health, Federal University of Technology Owerri, Imo State Nigeria.
Received : Oct 19, 2023 Accepted : Nov 17, 2023 Published : Nov 24, 2023
Epidemiology & Public Health - www.jpublichealth.org
Copyright: Innocent RC © All rights are reserved
Citation: Chukwuocha U, Charles GT, Innocent DC, Ogboeze JC, Innocent RC, et al. Perceived Experience and Management of Covid-19 in Southeastern Nigeria. Epidemiol Public Health. 2023; 1(3): 1023.
Abstract
SARS-CoV-2 causes the COVID-19 pandemic. Misconceptions and perceived experience with the onset of the COVID-19 infection are attributed to variations in symptom progression and a lack of timely diagnosis. This study aimed to identify the population of people in South-Eastern Nigeria who had perceived experience with and management of COVID-19. This population-based cross-sectional study of adult patients in South-Eastern Nigeria. Data from questionnaires were collected and statistically analyzed. Four hundred twenty responses were obtained, with 200(47.6%) respondents reporting perceived COVID-19 experience and 220(52.4%) reporting positive COVID-19 test results. The mean age of respondents with perceived experience was 37.61±12.27, while respondents with positive COVID-19 tests had a lower value (40.59±13.42). In comparison, 75.5% of respondents with perceived COVID-19 experience manifested unusual symptoms sequence, whereas this phenomenon was observed in 51.8% of positive COVID-19 patients. The most commonly reported symptoms are fever or chill (100% vs. 100%), cough (86% vs. 82%), and breathing difficulty (86% vs. 82%). Respondents with perceived COVID-19 experience primarily obtain their medication from a drug store (34.0%), whereas positive COVID-19 test respondents primarily obtain their medication from a hospital (64.1%). The study concluded that a lack of testing facilities could increase perceived experience with COVID-19, resulting in fewer people being tested for COVID-19. As a result, it is suggested that government agencies develop strategies to reduce the COVID-19 surge and improve testing facilities in southeastern Nigeria.
Keywords: COVID-19; Misconception; Perceived experience; Public health measures.
Introduction
In December 2019, an outbreak of the novel Coronavirus Disease 2019 (COVID-19), caused by Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2), was initially detected in Wuhan, China, which was then declared as the pandemic by the World Health Organization [1]. The virus has spread over many countries and territories leading to a significant impact as presented with a dramatic loss of human life, unprecedented challenge to public health, food systems supply problem, and the its socioeconomic consequences [2]. A person can be infected when virus-containing aerosols or droplets are inhaled directly or come into contact with the eyes, nose, skin, or mouth. The virus can also easily spread in poorly ventilated and/or crowded indoor settings [3].
The most common symptoms of COVID-19 include fever, fatigue, anorexia, cough, loss of taste, smell, and shortness of breath - but atypical manifestations of this virus continue to be reported and described [4]. Most people (81%) developed mild to moderate symptoms. In comparison, 14% develop severe symptoms (dyspnea, hypoxia, or more than 50% lung involvement on imaging), and 5% suffer critical symptoms (respiratory failure, shock, or multi-organ dysfunction) [5]. Moreover, at least a third of those infected with the virus remain asymptomatic and do not develop noticeable symptoms at any point in time, but they still can spread the disease [6].
Efforts have been put in place by the government and health policy makers to curb the spread of the virus by making policies and laws such as enacting of laws guiding the use of face masks, making policies as regards to precautionary measures such as observation of physical distancing, washing of hand, and use of hand sanitizers [3]. The procurement of COVID-19 vaccine by the government to vaccinate the public against the infection, yet this virus keeps ravaging and spreading throughout the world at large. While efforts have been placed on vaccinating the population, less attention has been paid as regards to the provision of testing facilities to diagnose the public on COVID-19 [1]. This has led to under-reporting of COVID-19 cases in the country and thus little or no interest in case finding and surveillance. Many who may have developed the signs and symptoms of COVID-19, manage the situation in an improper way [2].
Globally, COVID-19 continues to cause problems with scarcity of COVID-19 testing facilities is a major challenge in a bid to stop the spread of COVID-19 pandemic among the population especially in a developing country. [7] This has led to the less number of the population being tested of COVID-19, leaving the majority of the population untested of COVID-19, among the population that are untested are many who are positive of COVID-19. This is not encouraging considering the magnitude of the pandemic as it facilitates the spread of the virus among the population through symptomatic and asymptomatic transmission [8]. There is a possibility that many have been perceived to have COVID-19 through the manifestation of signs and symptoms of the diseases but due to lack of confirmatory tests many seek to take various health decisions which are detrimental to their health and that of the population at large in a bid to manage the situation. Lack of proper management of suspected COVID-19 may lead to the spread of the virus [9]. This study tends to study the population with perceived experience of COVID-19 and how they managed or are managing the disease. The general objective of the study is to determine the population of people with perceived experience and management of COVID-19 in South-Eastern Nigeria.
Methods
This population-based cross-sectional study was conducted in South-Eastern Nigeria to determine people perceived experience and management of COVID-19. All participants were the residents in various states aged 18 years and above and have lived for at least one year in the region of residence.
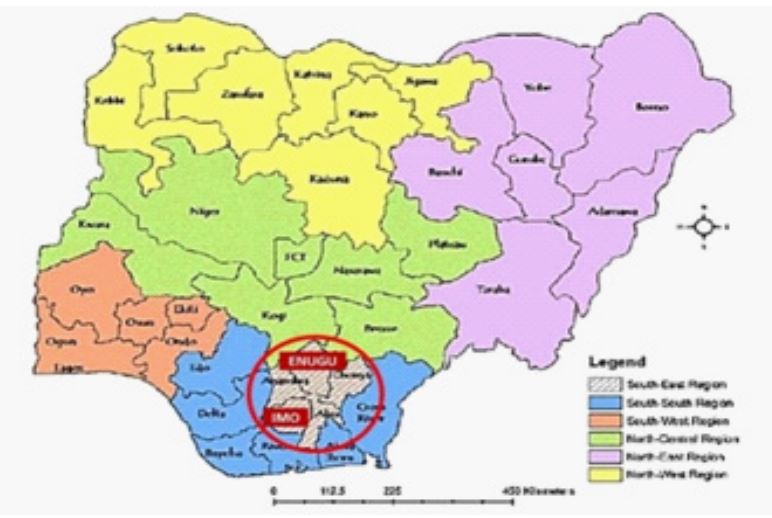
This research was conducted in the states of Enugu and Imo in South-Eastern Nigeria (Figure 1). The region is one of the most populous in the country, with an estimated 50,000,000 inhabitants in 2021, comparable to 25% of Nigeria’s population. The vast majority of people in this area are farmers, traders, artisans, civil servants, and students. The study area’s major activities are related to commercial, religious, educational, and social scope, which support the spread of COVID-19.
Sampling
The minimum sample size for the study would be calculated by using the following formula for comparison of two independent proportions:
n= (Zα + Zβ )2(p1q1+ p2q2)
(p1-p2)2
Where:
n = Minimum sample size for each group
p1 = Prevalence or proportion of the attribute present in the population 1 q1 = 1-p1
p2 = Prevalence or proportion of the attribute present in the population 2 q2 = 1-p2
Zα = Standard normal deviate corresponding to 95% level of significance (α) = 1.96
Zβ = Standard normal deviate corresponding to a power of 80% = 0.84
p1 = Proportion of perceived Experience of COVID-19 among Residents in a previous study = 50%.
p2 = Proportion of Confirmed Cases of COVID-19 in a previous study = 14.7%. If p1 = 50% = 0.50
Then q1 = 1-0.50 = 0.50
If p2 =14.7% = 0.147
Then q2 = 1-0.147 = 0.853
n= (1.96+ 0.84)2[(0.50)*(0.50)+(0.147)*(0.853)] / (0.50-0.147)2
n= 212.106 = 212
Adjusting for a 5% rate of non-response and invalid response (i.e 95% expected response rate = 0.95).
n= n/expected response rate
n= 212/0.95 = 223.15
n= 223
Therefore, a total of 223 questionnaires each would be distributed to both the population of people with perceived experience of COVID-19 and population with confirmed cases of COVID-19 in South-Eastern Nigeria.
Two states from South-Eastern Nigeria geopolitical landscape were selected using simple random sampling, while purposive sampling was used to sample the proportion of confirmed cases. An online (using Google form) or paper questionnaire was distributed to the selected states. Participants in the study were invited at random via various social media platforms such as Facebook, Twitter, Instagram, Whats App, and others via a Google form link leading to the e-questionnaire. In contrast, targeted participants, who have tested positive for COVID-19, were purposefully chosen for the study. They must agree and sign individual online-written informed consent following a proper introduction of the aim of the study by the researcher. Data collection was repeated until the appropriate sample size was obtained.
The researcher carefully prepared the questionnaire. Then, it was scrutinized by the researcher’s supervisor and an expert statistician. The reliability technique used in this study was a testretest approach to test the internal consistency of the research instrument. The questionnaire was given to 10 people who shared comparable research population characteristics but were not included in the study, and the process was repeated a week later. The Cronbach Alpha test was performed to examine the consistency of the results, and a coefficient of 0.8 was obtained.
Data analysis
The questionnaire data was imported into Microsoft Excel and analyzed with IBM SPSS Statistics for Windows, Version 22.0 (Armonk, NY: IBM Corp, 2013). To explain the data obtained, a descriptive statistical approach that included frequencies and percentages of distribution was utilized. Tables were prepared for all class variables and stated as distribution percentages. Association between variables were observed using Chi-square test (or Fisher exact in case of did not fulfill Chi-square requirement). The analysis was carried out at a 95% confidence interval, and the probability value was used to determine the strength of relationships, with values less than 0.05 being significant.
Ethics
A letter of introduction and ethical clearance was obtained from the Department of Public Health Ethical clearance committee in Federal University of Technology Owerri before the research was conducted. The purpose of the research was explained to each respondent and verbal informed consent was obtained from them before inclusion into the study. Also, anonymity of the respondents was assured and ensured. The confidentiality of the information they gave also maintained.
Results
Socio-demographic characteristics and travel history
Table 1 depicts the Socio-demographic characteristics of respondents with perceived experience of COVID-19 and those with confirmed positive COVID-19 tests. Respondents with perceived experience of COVID-19 have lower mean age than positive COVID-19 patients (37.61±12.27 vs. 40.59±13.42). Moreover, those with perceived experience of COVID-19 lie mainly in the 31-40 age group (31.0%), while in the positive COVID-19 group, dominant participants were 51 and above (35.0%). A statistically significant association was found between age group (p=0.003), gender (p=0.021), education (p=0.004), monthly household income (p=0.003), abroad travel history during the pandemic (p=0.002), and COVID-19 epicenter state visit (p<0.001) and the experience of COVID-19.
Table 1: Socio-demographic characteristics and travel history.
| Variables | Experience of COVID-19 | p-value | |
|---|---|---|---|
| Perceived | Confirmed | ||
| n=200 (%) | n=220(%) | ||
| Age group | |||
| Less than 20 | 20(10.0) | 20(9.1) | 0.003 |
| 21-30 | 34(17.0) | 22(10.0) | |
| 31-40 | 62(31.0) | 65(29.5) | |
| 41-50 | 51(25.5) | 36(16.4) | |
| 51 and above | 33(16.5) | 77(35.0) | |
| Gender | |||
| Female | 56(28.0) | 151(68.6) | 0.021 |
| Male | 144(72.0) | 69(31.4) | |
| Marital status | |||
| Married | 107(53.5) | 119(54.1) | 0.583 |
| Single | 74(37.0) | 74(33.6) | |
| Widowed | 19(9.5) | 27(12.3) | |
| Education | |||
| Non-formal education | 3(1.5) | 0(0.0) | 0.004 |
| Primary | 39(19.5) | 33(15.0) | |
| Secondary | 137(68.5) | 107(48.6) | |
| Tertiary | 21(10.5) | 80(36.4) | |
| Employment status | |||
| Employed | 168(84.0) | 195(88.6) | 0.076 |
| Unemployed | 1(0.5) | 4(1.8) | |
| Student | 28(14.0) | 21(9.5) | |
| Other | 3(1.5) | 0(0.0) | |
| Monthly house hold income | |||
| 3(1.5) | 0.003 | ||
| Less than 30,000 | 5(2.5) | 26(11.8) | |
| 30,000 – 49,000 | 33(16.5) | 15(6.8) | |
| 50,000 – 79,000 | 73(36.5) | 91(41.4) | |
| 80,000 – 100,000 | 82(41.0) | 48(21.8) | |
| Above 100,000 | 4(2.0) | 40(11.8) | |
| Traveled outside the country during the pandemic | |||
| No | 200(100) | 180(81.8) | 0.002 |
| Yes | 0(0.0) | 40(18.2) | |
| Visited any epicenter state | |||
| No | 164(82.0) | 135(61.4) | <0.001 |
| Yes | 36(18.0) | 85(38.6) | |
Table 2: Comparison of COVID-19 experience between respondents.
| Variables | Experience of COVID-19 | p-value | |
|---|---|---|---|
| Perceived | Confirmed | ||
| n = 200 (%) | n = 220(%) | ||
| Confirm experience with a test | |||
| No | 178(89.0) | 0(0.0) | 0.003 |
| Yes | 22(11.0) | 220(100.0) | |
|
Did the sequence of symptoms follow this
pattern? Fever →Cough →Sore throat →Headache →Muscle or body aches →Nausea or vomiting →Diarrhea |
|||
| No | 151(75.5) | 114(51.8) | 0.001 |
| Yes | 49(24.5) | 106(48.2) | |
| Experience loss of taste or smell | |||
| No | 173(86.5) | 145(65.9) | 0.001 |
| Yes | 27(13.5) | 75(34.1) | |
| Time taken to recover | |||
| Less than one week | 85(42.5) | 39(17.7) | 0.004 |
| One month | 6(3.0) | 30(13.6) | |
| One week | 14(7.0) | 13(5.9) | |
| Two weeks | 95(47.5) | 138(62.7) | |
| Hospitalized | |||
| No | 174(87.0) | 112(50.9) | <0.001 |
| Yes | 26(13.0) | 108(49.1) | |
Comparison of the COVID-19 experiences between respondents
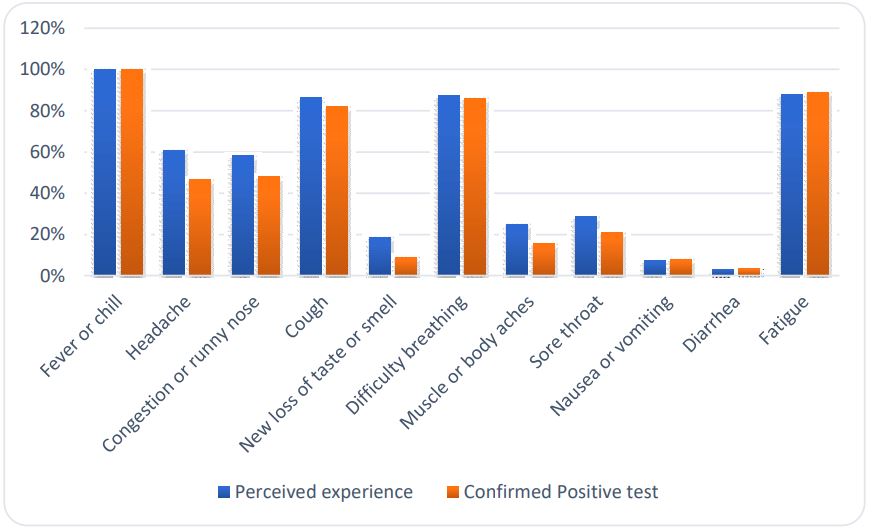
Figure 1 revealed the proportion of symptoms experienced by respondents. The most common symptoms in positive COVID-19 patients were fever or chill (100%), fatigue (88%), cough (86%), and breathing difficulty. A similar pattern was observed in perceived COVID-19 experience, with 100%, 89%, 82%, and 82%, respectively. However, it was later on described that the majority (89.0%) of those with perceived experience of COVID-19 have positive COVID-19 testing (Table 2). Table 2 shows a significant association between positive test confirmation of COVID-19 and the perceived experience of COVID-19 (p=0.003). In response to the sequence of symptoms pattern (Fever→Cough →Sore throat→Headache→Muscle or body aches→Nausea or vomiting→Diarrhea), 151(75.5%) of respondents with perceived experience COVID-19, while a similar phenomenon was found in 114 (51.8%) of participants with positive COVID-19. A statistically significant association was observed between the sequence of symptoms pattern (p=0.001), loss of taste or smell (P=0.001), the time of recovery (p=0.004), and hospitalization (p<0.001) with the experience of COVID-19.
Table 3: Comparison of the management of COVID-19 among respondents.
| Variables | Experience of COVID-19 | p-value | |
|---|---|---|---|
| Perceived | Confirmed | ||
| n = 200 (%) | n = 220(%) | ||
| First action following symptoms development | |||
| Called a health practitioner | 23 (11.5) | 4 (1.8) | 0.002 |
| No action was taken | 96 (48.0) | 0 (0.0) | |
| Self-medication | 1 (0.5) | 1 (0.45) | |
| Visited the drug shop | 43 (21.5) | 122 (55.5) | |
| Went to the hospital | 37 (18.5) | 92 (42.3) | |
| Self-isolation practice | |||
| No | 200 (100) | 86 (39.1) | 0.001 |
| Yes | 0 (0.0) | 134 (60.9) | |
| Medication consumption | |||
| No | 97 (48.5) | 0 (0.0) | 0.004 |
| Yes | 103 (51.5) | 220 (100.0) | |
| Place where the medication was obtained | |||
| Took No action | 96 (48.0) | 0 (0.0) | |
| Drug shop | 68 (34.0) | 79 (35.9) | |
| Hospital | 32 (16.0) | 141 (64.1) | 0.003 |
| Leftover drugs | 1 (0.5) | 0 (0.0) | |
| Other | 3 (1.5) | 0 (0.0) | |
| Drug prescriber | |||
| No Action was taken | 97 (48.5) | - | |
| Drug vendors | 28 (14.0) | 54 (24.5) | 0.093 |
| Medical doctors | 46 (23.0) | 153 (69.5) | |
| Self-prescription | 12 (6.0) | 2 (0.9) | |
| Relatives | 16 (8.0) | 11 (5.0) | |
| Other | 1 (0.5) | 0 (0.0) | |
| Prescription method | |||
| No consumption | 97 (48.5) | 0 (0.0) | |
| Face to face at home | 22 (11.0) | 44 (20.0) | 0.092 |
| Face to face at the hospital | 56 (28.0) | 152 (69.1) | |
| Over the phone | 23 (11.5) | 24 (0.9) | |
| Others | 2 (1.0) | 0 (0.0) | |
Comparison of COVID-19 management
The two most common medications consumed by the participants are vitamin C and Zinc. Vitamin C was consumed by 80% of perceived experience participants, while Zinc was consumed by 16% of participants. Similarly, vitamin C (77%) and Zinc (14%) were consumed by positive COVID-19 participants. However, 65% of respondents with perceived experience and 68% with positive COVID-19 test have no idea about the type of medication consumption (Figure 2).
Table 3 shows the management of COVID-19 among respondents. Those with perceived experience of COVID-19 preferred no action (48%) or visited the drug shop (21.5%). Meanwhile, respondents with positive COVID-19 tests visited the drug shop (55.5%) or went to the hospital (42.3%). A significant association was established between the first action taken by respondents and the experience of COVID-19 (p=0.002), self-isolation practice (p=0.001), and medication consumption (p=0.004) and the experience of COVID-19 (P=0.092).
Discussion
Our study depicts that the age mostly affected by COVID-19 perceived experience is usually above the youth age. This is in line with a previous report demonstrating that the SARS Cov-2 affects people aged 40 years and above [10]. We also found that travel history has significant association with COVID-19 case. This is also revealed by a study which stated that travel history is considered as a risk factor for COVID-19 infection [11].
Most participants with perceived COVID-19 experience (89.0%) did not confirm their experience with a test. This ascertains and justifies the general objective of this study. A recent publication by stated that symptomatic pattern and various body changes influence the mind prediction towards an infection [12]. Furthermore, individuals with perceived experience of COVID-19 are more likely to presume infection in responses to the sequence of symptom patterns. Based on the comparison on the infectious pattern from the study it was demonstrated that Fever →Cough →Sore throat →Headache →Muscle or body aches →Nausea or vomiting → Diarrhea was the observed pattern and more than three-fourth of respondents with perceived experience COVID-19 have unusual symptom pattern development. One of the most important contributor of this condition is greater anxiety and depressive symptoms among people with high risk of infection [13]. According to a report, South-Eastern Nigeria has less equipped facilities for managing and treating patients with COVID-19 [14]. Thus majority of the individuals with perceived experience of COVID-19 are more likely to opt for other alternatives due to lack of clinical diagnosis including the search of traditional herbs, as mentioned with similar previous study [15].
Concerning the management of COVID-19 among respondents with perceived experience of COVID-19 and those with confirmed positive COVID-19 test, our study found that 11.5% of respondents with perceived experience of COVID-19 called a health practitioner, in contrast to a study which found that 48% residents with pneumonia called for medical attention in hospital [16]. Contradictorily, only 1.8% of respondents with positive COVID-19 test called a health practitioner, which could be attributed to the study’s location [17]. We also found that 51.5% of respondents with perceived COVID-19 experience took medication, while all respondents with confirmed positive COVID-19 test took medication. This could be because respondents’ actions and decisions are hampered by their perceived experience [18]. This report is consistent with the study on COVID-19 management among respondents with perceived COVID-19 experiences. Furthermore, respondents with perceived COVID-19 experience obtain their medication mainly from a drug store (34.0%), whereas respondents with confirmed positive COVID-19 test obtain their medication from hospital (64.1%). This demonstrates that individuals with perceived COVID-19 experience in southeastern Nigeria used drug stores to make COVID-19 drug choices, which is also observed as one of the most common method in previous study [19].
Conclusion
This study concludes that despite the efforts made by concerned organizations on the management of COVID-19 in Nigeria, it has been seen that a lack of testing facilities could increase perceived experience towards COVID-19 without a timely diagnosis, and this has led to a less number of the population being tested of COVID-19, leaving the majority of the population untested of COVID-19, among the untested population are many who are positive of COVID-19. The government and concern agencies in Southeastern Nigeria can act with world bodies to minimize misconceptions due to the pandemic because it influences the perceived experience and management options of individuals in a community. Future studies must be placed on the significant gaps and constraints in identifying the various groups in the study. Furthermore, effective and efficient training should be provided to the concerned stakeholders on communication and measures to reduce morbidity and assure public safety.
Declarations
Ethics approval and consent to participate: Not applicable.
Consent to publish: Not applicable.
Availability of data and materials: The data set from the study are available to the corresponding author upon request.
Competing interests: Authors have declared that they have no competing interests.
Funding: No funds were received for this study.
Acknowledgements: Not applicable.
References
- Farahat RA, Abdelaal A, Umar TP, El-Sakka AA, Benmelouka AY, et al. The emergence of SARS-CoV-2 Omicron subvariants: current situation and future trends. Le Infez Med. 2022; 30: 480.
- Jain N, Hung IC, Kimura H, Goh YL, Jau W, et al. The global response: How cities and provinces around the globe tackled covid-19 outbreaks in 2021. Lancet Reg Heal Asia. 2022; 4: 100031.
- Farahat RA, Baklola M, Umar TP, Omicron B. 1.1.529 subvariant: Brief evidence and future prospects. Ann Med Surg. 2022; 83: 104808.
- Baj J, Karakuła Juchnowicz H, Teresiński G, Buszewicz G, Ciesielka M, et al. COVID-19: Specific and Non-Specific Clinical Manifestations and Symptoms: The Current State of Knowledge. Journal of Clinical Medicine. 2020; 9: 1753.
- Wu Z, McGoogan JM. Characteristics of and important lessons from the coronavirus disease 2019 (COVID-19) outbreak in China: Summary of a report of 72 314 cases from the Chinese Center for Disease Control and Prevention. Jama. 2020; 323: 1239–1242.
- Oran DP, Topol EJ. The Proportion of SARS-CoV-2 Infections That Are Asymptomatic : A Systematic Review. Ann Intern Med. 2021; 174: 655–662.
- Hyland Wood B, Gardner J, Leask J, Ecker UKH, et al. Toward effective government communication strategies in the era of COVID-19. Humanit Soc Sci Commun. 2021; 8: 30.
- Shereen MA, Khana S, Kazmi A, Bashir N, Siddique R, et al. COVID-19 infection: Origin, transmission, and characteristics of human coronaviruses. J Adv Res. 2020; 24: 91–98.
- Chemali S, Mari Sáez A, El Bcheraoui C, Weishaar H. Health care workers’ experiences during the COVID-19 pandemic: A scoping review. Hum Resour Health. 2022; 20: 27.
- Levin AT, Hanage WP, Owusu-Boaitey N, Cochran KB, Walsh SP, et al. Assessing the age specificity of infection fatality rates for COVID-19: Systematic review, meta-analysis, and public policy implications. Eur J Epidemiol. 2020; 35: 1123–1138.
- McClymont H, Hu W. Weather variability and COVID-19 transmission: A review of recent research. Int J Environ Res Public Health. 2021; 18: 396.
- Rodríguez Rey R, Garrido Hernansaiz H, Collado S. Psychological Impact and Associated Factors During the Initial Stage of the Coronavirus (COVID-19) Pandemic Among the General Population in Spain. Front Psychol. 2020; 11: 1540.
- Sherman AC, Park CL, Salsman JM, Williams ML, Amick BC, Hudson TJ, et al. Anxiety, depressive, and trauma symptoms during the COVID-19 pandemic: Evaluating the role of disappointment with God. J Affect Disord. 2021; 293: 245–253.
- Iwuoha VC, Aniche ET, Obiora CA, Umeifekwem UT. Citizens lack access to healthcare facilities: How COVID-19 lockdown and social distancing policies boost roadside chemist businesses in South-Eastern Nigeria. Int J Health Plann Manage. 2021; 36: 2411–2423.
- Lam CS, Koon HK, Chung VC-H, Cheung YT. A public survey of traditional, complementary and integrative medicine use during the COVID-19 outbreak in Hong Kong. PLoS One. 2021; 16: e0253890.
- Burton DC, Flannery B, Onyango B, Larson C, Alaii J, et al. Healthcare-seeking behaviour for common infectious disease-related illnesses in rural Kenya: a community-based house-to-house survey. J Health Popul Nutr. 2011; 29: 61–70.
- Yusefi AR, Sharifi M, Nasabi N sadat, Rezabeigi Davarani E, Bastani P. Health human resources challenges during COVID-19 pandemic; Evidence of a qualitative study in a developing country. PLoS One. 2022; 17: e0262887.
- Rieckert A, Teichmann A-L, Drewelow E, Kriechmayr C, Piccoliori G, et al. Reduction of inappropriate medication in older populations by electronic decision support (the PRIMA-eDS project): A survey of general practitioners’ experiences. J Am Med Inform Assoc. 2019; 26: 1323–1332.
- Susilo AI, Muslim Z. Community Behavior Study Regarding Drug Purchases at Bengkulu City Pharmacies in 2021. SANITAS J Teknol dan Seni Kesehat. 2022; 13: 33–43.