
Research ArticleOpen Access, Volume 1 Issue 2
Knowledge of Skin Diseases and Associated Risk Factors among Students of a Public Secondary School in Ekiti State, Nigeria
Richard Dele Agbana1; Opeyemi Oladipupo Abioye2*; Tope Michael Ipinnimo2; Demilade Olusola Ibirongbe3; Elijah Olusegun Elegbede2
1Department of Community Medicine, Afe Babalola University, Ado-Ekiti, Nigeria.
2Department of Community Medicine, Federal Teaching Hospital, Ido-Ekiti, Nigeria.
3Department of Community Medicine, University of Medical Sciences, Ondo, Nigeria.
*Corresponding author: Opeyemi Oladipupo Abioye
Department of Community Medicine, Federal Teaching Hospital, Ido-Ekiti, Nigeria.
Received : Oct 21, 2023 Accepted : Nov 07, 2023 Published : Nov 14, 2023
Epidemiology & Public Health - www.jpublichealth.org
Copyright: Abioye OO © All rights are reserved
Citation: Agbana RD, Abioye OO, Ipinnimo TM, Ibirongbe DO, Elegbede EO, et al. Knowledge of Skin Diseases and Associated Risk Factors among Students of a Public Secondary School in Ekiti State, Nigeria. Epidemiol Public Health. 2023; 1(2): 1020.
Abstract
Introduction: Physiological and structural differentiation of the pilosebaceous unit occur typically in general population, such changes are usually very prominent in adolescents with increased sebaceous and apocrine secretions. Knowledge of such changes and associated factors has not been adequately described among secondary school students in Nigeria.
Methods: This descriptive cross-sectional study was conducted among public secondary school students of Federal Teaching Hospital, Ido-Ekiti (FETHI) Staff School. All data collected were analyzed with IBM version 25.0. Chi-square test and binary logistic regression were used in bivariate and multivariate analyses to determine significance. P<0.05 was taken as significant.
Results: Majority of the respondents were aged between 9-15 years (86.5%) with males accounting for 50.7%. Respondents in JSS 2 class have a lesser odd (OR = 0.090; 95% CI = 0.015-0.540) of having good knowledge of skin diseases than those in SSS 3 class. Respondents which reported twice daily bathing (OR = 5.418; 95%CI = 1.295-22.679), those that took measures to prevent skin diseases (OR = 6.870; 95% CI = 2.936-16.076), and those that have been previously treated for a skin condition (OR=2.825; 95% CI = 1.017-7.846) have higher odds of having good knowledge of skin disease.
Conclusion: The study discovered appreciable knowledge of skin diseases among the students, such knowledge was associated with being in lower class, higher number of bathing times at least twice daily, good awareness of skin diseases, taking measures to prevent skin diseases, and previous treatment of any skin disease.
Keywords: Knowledge; Skin diseases; Risk factors; Students.
Introduction
Physiological and structural differentiation of the pilosebaceous unit occur typically in general population, such changes are usually very prominent in adolescents with increased sebaceous and apocrine secretion [1]. The knowledge of such changes, associated factors, and resultant pathologies have not been adequately described among secondary school students in Nigeria though it is well established in United States of America that 1 in 3 persons would have come down with skin condition in a life time [2]. The totality of skin conditions world-wide were noted to be number four among non-fatal disease burden, and the negative outlook of skin conditions was high in both developed and emerging economies, emphasizing the need for prioritization of skin disease prevention [3]. This high burden does not exclude secondary school students but cut across all human age groups [3]. Knowledge about the burden of various skin conditions and associated risk factors promotes appropriate planning and the provision of care on tackling these problems [4], hence the need to look into the level of knowledge and awareness about skin diseases among students. Several developing nations are still plagued by the vicious cycle of ignorance, deprivation, and sickness, which significantly contributes to the incidence of numerous skin disorders [5]. Most of these skin diseases thrive best in settings where ignorance and poverty are intertwined due to a lack of health education, the neglect of personal health as a result of unsanitary living conditions, a lack of funds to buy prescribed drugs, and unconventional health consultations and treatments, or in settings where the general health of the population is endangered by the local health authority’s misplaced priorities [5].
Different risk factors, such as genetics, racial makeup, social and hygienic standards, customs and occupations, nutritional status, age structure of the community, climatic factors, level of industrialization, and the quality and quantity of medical care, can affect the prevalence of skin diseases in any community [6]. Risk factors may not be causal in skin disease pathophysiology but can be associated with early pathological skin manifestations in secondary school students. Prompt identification of such risks in peripubertal age group will promote better and excellent skin outcomes in the nearest future.
A comprehensive survey of general practitioners’ workloads in Australia revealed skin problems were the primary reason for at least 15% of consultations, where as a community-based data collections show that physicians are consulted about skin conditions by less than 50% of those with skin pathologies and majority of people seek advice from pharmacists, family or friends and naturopaths or they simply carry out self-prescription based on non-valid information and low knowledge on skin conditions [7]. It is pertinent to reduce the total number of years lived with disability among the upcoming generation in the tropics (Nigeria inclusive) as skin infections resulted in large amount of YLD (Years of life Lived with Disability) in tropical and low-resource countries, and eczema responsible for a large part of YLD in all continents [3]. A study done in Ilorin Kwara state Nigeria revealed a high prevalence (66.5%) of skin diseases among public secondary school students which could have resulted from low knowledge about such conditions among the students [8]. The aim of this study was to assess knowledge of skin diseases and associated factors among students in a public secondary school in Ekiti state, Nigeria.
Methods
This study was conducted among junior and senior secondary school students of Federal Teaching Hospital Ido-Ekiti (FETHI) Staff School. The school was founded in 2010 to cater for the secondary education of the children of staff of the Federal Teaching Hospital, Ido-Ekiti. However, the school is also open to children of non-staff members of the community. It is a day school with no boarding house facility. The school currently has a total of 245 students that are majorly adolescents with an average of 24 students in a class.
This study utilized descriptive cross-sectional analysis to determine the knowledge of skin disease among the students. The study population included all the students of FETHI Staff School. None-consenting and students who were absent from school on data collection days were excluded from the study.
The whole student population of the school was recruited for the study. A comprehensive list of all the students was developed according to their class ranging from Junior Secondary School (JSS) 1, JSS2, JSS3, Senior Secondary School (SSS)1, SSS2, to SSS3. Relevant data were collected from all the enlisted students with the aid of an interviewer-administered semi-structured questionnaire. Final year medical students of a nearby university who were trained as research assistants on how to appropriately administer the questionnaire carried out the data collection.
The study instrument was designed by the researchers after extensive literature review, and pre-tested in another public secondary school in Ido-Ekiti. Face and content validity of the instrument was done by Experts in the Community Medicine Department and Dermatology Unit of Federal Teaching Hospital, Ido-Ekiti. Data were collected on the socio-demographic characteristics, hygiene, and other student factors for skin diseases as well as knowledge of skin disease. Consent and child assent was taken prior to the administration of the questionnaire.
All data collected were analyzed with IBM version 25.0. Knowledge was presented using a bar chart, percentages and frequency tables were used to present other categorical variables. Chi-square test and binary logistic regression were used in bivariate and multivariate analyses to determine significance. P<0.05 was taken as significant.
Ethical approval to conduct study was sought and obtained from the Federal Teaching Hospitals’ Health Research and Ethical Committee (HREC).
Results
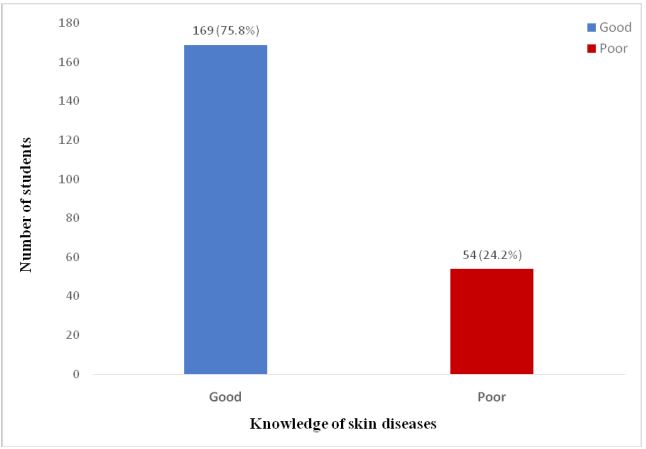
Out of a total of 245 potential respondents in the school, 223 were available, consented and responded with complete data. The majority of the respondents were aged between 9-15 years (86.5%) with males accounting for 50.7% of them. The majority were of Yoruba tribe (87.0%) and practice Christianity (96.4%). Figure 1 shows the knowledge of skin diseases among the respondents where 75.8% of them had good knowledge and 24.2% had poor knowledge.
Table 1 shows the association between socio-demographic variables and knowledge of skin diseases among the respondents. There was a significant association between class and knowledge of skin disease (p<0.001). Table 2 reveals that the number of bathing times was significantly associated with knowledge of skin disease among the respondents (p<0.014).It was also revealed in Table 3 that awareness of skin diseases (p<0.001), taking measures to prevent skin diseases (p<0.001) and previous treatment of any skin condition (p<0.008) was significantly associated with knowledge of skin disease among the respondents.
Table 1: Association between socio-demographic variable and knowledge of skin diseases.
| Knowledge of skin disease | |||||
|---|---|---|---|---|---|
| Good | Poor | Total | χ2 | p value | |
| Variables | n(%) | n(%) | N(%) | ||
| Age group (years) | |||||
| 9-15 | 144(74.6) | 49(25.4) | 193 | 1.076 | 0.300 |
| 16-20 | 25(83.3) | 5(16.7) | 30 | ||
| Sex | |||||
| Male | 86(76.1) | 27(23.9) | 113 | 0.013 | 0.910 |
| Female | 83(75.5) | 27(24.5) | 110 | ||
| Class | |||||
| JSS1 | 23(52.3) | 21(47.7) | 44 | 44.891 | <0.001 |
| JSS2 | 20(50.0) | 20(50.0) | 40 | ||
| JSS3 | 41(87.2) | 6(12.8) | 47 | ||
| SS1 | 30(93.8) | 2(6.3) | 32 | ||
| SS2 | 32(91.4) | 3(8.6) | 35 | ||
| SS3 | 23(92.0) | 2(8.0) | 25 | ||
| Tribe | |||||
| Yoruba | 147(75.8) | 47(24.2) | 194 | 0.000 | 0.992 |
| Others | 22(75.9) | 7(24.1) | 29 | ||
| Religion | |||||
| Christianity | 161(74.9) | 54(25.1) | 215 | 2.651F | 0.204 |
| Islam | 8(100.0) | 0(0.0) | 8 | ||
| Family type | |||||
| Monogamy | 153(76.1) | 48(23.9) | 201 | 0.124F | 0.794 |
| Polygamy | 16(72.7) | 6(27.3) | 22 | ||
Table 2: Association between hygiene factors and knowledge of skin diseases.
| Knowledge of skin diseases | |||||
|---|---|---|---|---|---|
| Good | Poor | Total | χ2 | p value | |
| Variables | n(%) | n(%) | N(%) | ||
| Bathing water | |||||
| River | 5(71.4) | 2(28.6) | 7 | 0.693 | 0.707 |
| Well | 57(79.2) | 15(20.8) | 72 | ||
| Tap | 107(74.3) | 37(25.7) | 144 | ||
| Number of bathing times | |||||
| 1 | 43(72.9) | 16(27.1) | 59 | 8.553 | 0.014 |
| 2 | 119(79.9) | 30(20.1) | 149 | ||
| >2 | 7(46.7) | 8(53.3) | 15 | ||
| Use of soap for bathing | |||||
| Yes | 166(76.9) | 50(23.1) | 216 | 4.270F | 0.061 |
| No | 3(42.9) | 4(57.1) | 7 | ||
| Number of people in room with respondent | |||||
| None | 9(90.0) | 1(10.0) | 10 | 7.813F | 0.138 |
| 1 | 97(80.8) | 23(19.2) | 120 | ||
| 2 | 40(64.5) | 22(25.0) | 62 | ||
| 3 | 15(75.0) | 5(25.0) | 20 | ||
| 4 | 7(77.8) | 2(22.2) | 9 | ||
| ≥ | 5 | 1(50.0) | 1(50.0) | 2 | |
| Sweats excessively | |||||
| Yes | 57(71.3) | 23(28.7) | 80 | 1.398 | 0.237 |
| No | 112(78.3) | 31(21.7) | 143 | ||
| How do you clean your sweat? | |||||
| Face Towel | 118(77.1) | 35(22.9) | 153 | 4.953F | 0.164 |
| Hand Wipe | 35(77.8) | 10(22.2) | 45 | ||
| T-Shirt | 7(50.0) | 7(50.0) | 14 | ||
| Do not clean routinely | 9(81.8) | 2(18.2) | 11 | ||
| Do you share personal items? | |||||
| Yes | 60(75.9) | 19(24.1) | 79 | 0.002 | 0.966 |
| No | 109(75.7) | 35(24.3) | 144 | ||
| Use of skin lightening cream | |||||
| Yes | 35(71.4) | 14(28.6) | 49 | 0.649 | 0.420 |
| No | 134(77.0) | 40(23.0) | 174 | ||
χ2: Chi square test; p value: < 0.05.
Table 4 shows the result of the binary logistic regression of independent predictors of knowledge of skin diseases. Respondents in JSS 2 class have a lesser odd (OR=0.090; 95% CI=0.015- 0.540) of having good knowledge of skin diseases than those in SSS 3 class. Also, respondents that reported twice daily bathing (OR=5.418; 95% CI=1.295-22.679), those that took measures to prevent skin diseases (OR=6.870; 95% CI=2.936-16.076), and those that have been previously treated for a skin condition (OR=2.825; 95% CI=1.017-7.846) have higher odds of having good knowledge of skin disease.
Table 3: Association between other factors and knowledge of skin diseases.
| Knowledge of skin diseases | |||||
|---|---|---|---|---|---|
| Good | Poor | Total | χ2 | p value | |
| Variables | n (%) | n (%) | N (%) | ||
| Aware of skin diseases | |||||
| Yes | 140(87.5) | 20(12.5) | 160 | 42.356 | <0.001 |
| No | 29(46.0) | 34(54.0) | 63 | ||
| Takes measures to prevent skin disease | |||||
| Yes | 132(89.2) | 16(10.8) | 148 | 43.086 | <0.001 |
| No | 37(49.3) | 38(50.7) | 75 | ||
| History of food or drug allergy | |||||
| Yes | 46(82.1) | 10(17.9) | 56 | 1.647 | 0.199 |
| No | 123(73.7) | 44(26.3) | 167 | ||
| Ever been treated for any skin condition | |||||
| Yes | 57(87.7) | 8(12.3) | 65 | 7.088 | 0.008 |
| No | 112(70.9) | 46(29.1) | 158 | ||
| Family history of skin disease | |||||
| Yes | 17(77.3) | 5(22.7) | 22 | 0.029 | 0.864 |
| No | 152(75.6) | 49(24.4) | 201 | ||
χ2: Chi square test; p value: < 0.05.
Table 4: Binary logistic regression of predictors of good knowledge of skin diseases.
| Variable | B | OR | 95% CI | p value | |
|---|---|---|---|---|---|
| Lower | Upper | ||||
| Class | |||||
| JSS1 | -1.448 | 0.235 | 0.038 | 1.459 | 0.120 |
| JSS2 | -2.412 | 0.090 | 0.015 | 0.540 | 0.008 |
| JSS3 | -0.821 | 0.440 | 0.067 | 2.897 | 0.393 |
| SS1 | -0.057 | 0.945 | 0.097 | 9.170 | 0.961 |
| SS2 | -0.283 | 0.754 | 0.093 | 6.129 | 0.792 |
| SS3 Ref | 1 | ||||
| Number of bathing times | |||||
| 1 | 1.133 | 3.106 | 0.681 | 14.162 | 0.143 |
| 2 | 1.690 | 5.418 | 1.295 | 22.679 | 0.021 |
| > 2 Ref | 1 | ||||
| Aware of skin diseases | |||||
| Yes | 0.805 | 0.009 | 2.236 | 1.227 | 4.076 |
| NoRef | 1 | ||||
| Takes measures to prevent skin disease | |||||
| Yes | 1.927 | 6.870 | 2.936 | 16.076 | <0.001 |
| No | 1 | ||||
| Ever been treated for any skin condition | |||||
| Yes | 1.038 | 2.825 | 1.017 | 7.846 | 0.046 |
| NoRef | 1 | ||||
χ2: Chi square test; p value: < 0.05.
Discussion
The study was carried out among secondary school students of a public secondary school in Ido-Ekiti, Nigeria. The sample population belonged to adolescent age group and such age group requires early sensitization on dermatological health practices to avert eventful skin outcomes in the nearest future. In this study, 75.8% of the respondents had good knowledge of skin diseases while 24.2% had poor knowledge of skin diseases, a study in Thailand among adolescents also showed a similar high score (95%) on impressive display of knowledge on skin care and diseases [9]. Another study in Thailand on knowledge of skin care revealed that male respondents had less basic knowledge about photo-protection than their female counter parts, also males knew significantly less than females about the effect of the sunlight on the skin and performed sun protection commendably less often than females [9]. Similar to our findings in this study, high school students in Thailand had significantly more appropriate knowledge about skin disease in relation to photo-protection than junior school students [9].
Such good knowledge amongst the respondents may be attributed to the fact that majority of the students have parents who belonged to the health work force, hence such skin health care knowledge could have been passed to their wards at home. Factors associated with knowledge of skin disease include class (especially lower class JSS 2), the number of bathing times, awareness of skin diseases, taking measures to prevent skin diseases, and previous treatment of any skin disease among the respondents. Lower class students may not be conscious of their skin outward looks as senior class students because majority of such lower class students are in early phase of puberty characterized by lower attention to physical attraction and aesthetics compared to their senior class counterparts who are in late puberty and are fully conscious of their looks and outward beauty as this can be supported by the finding in Thai where teenagers in senior high school used skin care products significantly more often than teenagers in junior high school as a result of acne [4]. Major 87.5% of respondents had good awareness on skin diseases while 99.5% among Thai adolescents had greater awareness than the Nigerian study counterpart, [4]this can be attributed to racial and cultural differences between the adolescent subjects. A similar study in Mauritius among adolescents revealed higher number of respondents (89%) being fully aware of the impact humidity can have on the skin, hence they did not keep their clothes in a humid environment [10]. A study in Maiduguri, North Eastern Nigeria discovered that majority (95.7%) of respondents had good knowledge on skin whitening agents like mercury, hydroquinone, and corticosteroid, while 43.9% of them got to know about the active ingredients in skin whitening creams via reading the leaflets (21.2%) or being told by close allies (17.2%) [10]. However, a contrary finding was identified among Thai adolescents where being previously treated for skin disease was not associated with knowledge [4].
Predictors of good knowledge among respondents include being a member of (lower) JSS2 class, bathing at least two times daily, taking measure to prevent skin disease, and being treated for a skin disease before the study. Though sex as a factor in this study wasn’t significant but it was discovered in Ilorin among secondary school students that skin disorders were commoner in females, also students attending public schools, students in the senior secondary classes, also mid-adolescents this was contrary to our findings probably because of parental influence on female students in the secondary in Ekiti whose parents are majorly literate belonging to health workers category unlike in Ilorin where most of the public school students might have come from parents who are illiterate traders [8]. Another study in Sagamu discovered male sex (twice likely to develop skin disease than females), having siblings greater four in number, and previous skin disease to be strong determinants of skin disorders among subjects in public school [12]. Reporting to have been previously treated on skin disease was found to be one of the strong predictors of having good knowledge of disease, this is similar to Sagamu study that discovered previous skin disease as a determinant of developing skin disease [12].
Conclusion and recommendation
The study discovered appreciable knowledge of skin diseases among the students; such knowledge was associated with being in lower class, higher number of bathing times at least twice daily, good awareness of skin diseases, taking measures to prevent skin diseases, and previous treatment of any skin disease. It is recommended that appropriate health intervention taking into cognizance risk factors for skin disease be targeted among this population group.
References
- Alshamrani HM, Alsolami MA, Alshehri AM, Salman AK, Alharbi MW, et al. Pattern of skin diseases in a university hospital in Jeddah, Saudi Arabia: Age and sex distribution. Annals of Saudi Medicine. 2019; 39: 22-28.
- Bickers DR, Lim HW, Margolis D, Weinstock MA, Goodman C, et al. The burden of skin diseases: 2004: A joint project of the American Academy of Dermatology Association and the Society for Investigative Dermatology. Journal of the American Academy of Dermatology. 2006; 55: 490-500.
- Hollestein LM, Nijsten T. An insight into the global burden of skin diseases. J Invest Dermatol. 2014; 134: 1499–1501.
- Al-Saeed WY, Al-Dawood KM, Bukhari IA, Bahnassy AA. Risk factors and co-morbidity of skin disorders among female schoolchildren in Eastern Saudi Arabia. Investigacion clinica. 2007; 48: 199-212.
- Onayemi O, Isezuo SA, Njoku CH. Prevalence of different skin conditions in an outpatients’ setting in north western Nigeria. International journal of dermatology. 2005; 44: 7-11.
- Al-Saeed WY, Al-Dawood KM, Bukhari IA, Bahnassy AA, et al. Risk factors and co-morbidity of skin disorders among female schoolchildren in Eastern Saudi Arabia. Investigacion clinica. 2007; 48: 199-212.
- Wohl Y, Freidman T, Brenner S, Bar Dayan Y, et al. Screening for common dermatologic disorders amongst Israeli adolescents. Int J Dermatol. 2007; 46: 1046–1049.
- Oyedepo JT, Katibi OS, Adedoyin OT. Cutaneous disorders of adolescence among Nigerian secondary school students. Pan Afr Med J. 2020; 36: 1–10.
- Nitiyarom R, Banomyong N, Wisuthsarewong W. Knowledge about, attitude toward, and practices in skin care among Thai adolescents. J Cosmet Dermatol. 2022; 21: 1539–1546.
- Kawshar T, Rajesh J. Sociodemographic factors and their association to prevalence of skin diseases among adolescents. Our Dermatology Online/Nasza Dermatologia Online. 2013; 4.
- Amodu MO, Bolori MT, Ahmad IM, Kale A, Kuchichi A, et al. Knowledge, Attitude and Practice of Skin Whitening among Female University Students in Northeastern Nigeria. OALib. 2018; 05: 1–14.
- Amoran OE, Runsewe-Abiodun OO, Mautin AO, Amoran IO. Determinants of dermatological disorders among school children in Sagamu, Nigeria. Educ Res. 2011; 1743-1748.